 Therapeutic
Intranasal Drug Delivery
Therapeutic
Intranasal Drug DeliveryIntranasal Medications for acute pain:
Table of Contents:
Introduction to nasal opiates for treatment of acute pain (click here)
Advantages of intranasal opiate medications (click here)
Concerns regarding intranasal opiate medications (click here)
Therapeutic threshold, side effect threshold (click here)
Literature overview and discussion
Pediatric pre-operative and post-operative agitation/pain control (click here)
Adult Postoperative pain control (click here)
Intranasal ketorolac (Toradol) in the operating suite (click here)
Acute pain in the Emergency department and prehospital setting
Intranasal opiates (fentanyl , diamorphine) for painful pediatric injuries (click here)
Intranasal opiates (fentanyl) for adult ambulance patients (click here)
Intranasal opiates (diamorphine, fentanyl) for sickle cell crisis (click here)
Intranasal opiates (fentanyl) for burn dressing changes (click here)
Intranasal Ketamine for acute pain (click here)
Intranasal flumazenil and intranasal naloxone as a reversal agents (click here)
Personal insights from experienced clinicians (click here)
Treatment protocol (click here)
Dosing tables (to assist with volume calculations) (click here)
Teaching materials (click here)
Peer Reviewed Articles (click here)
Introduction
Intranasal opiate delivery offers one of the most interesting and perhaps broadly useful indications for intranasal medication delivery. Acute pain is an extremely common problem in the outpatient setting (over 40 million emergency room visits in the United States per year for acute pain),[1] as well as in the hospice setting where patients often have acute episodes of breakthrough pain despite long acting opioid use. Due to the sheer volume and variety of patients a large number of treatment options are necessary to meet each patients individual needs.
Intranasal opiates are simply one of many treatment options that may be useful in selected patients. For selected opiate medications, intranasal delivery can result in rapid medication absorption with serum and cerebral spinal fluid (CSF) levels approaching those comparable to intravenous (IV) administration.
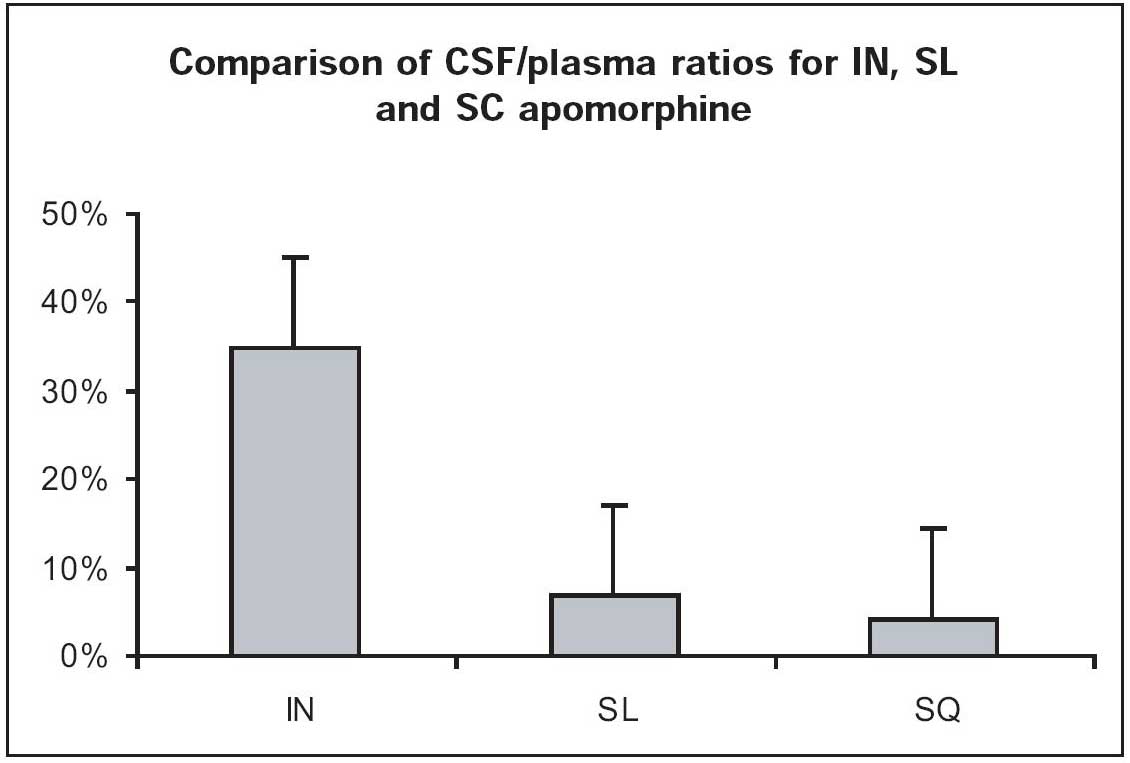
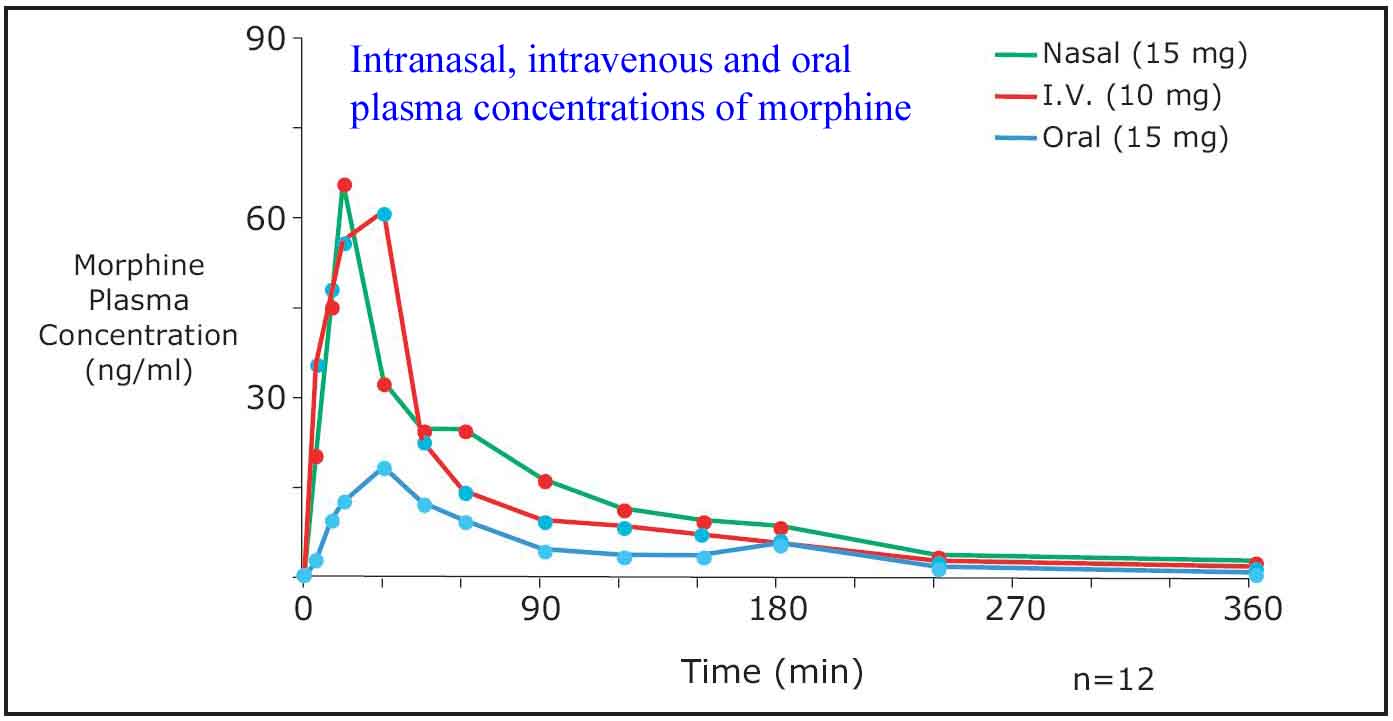
This delivery method is effective because the enormous surface area (180 cm2) and blood supply of the mucosa allows small molecules to be rapidly transported into the blood stream.[2] For example, dipping a cotton swab tip into sufentanil and applying it to the nasal mucosa of the ferret produces an effect within seconds.[2] Recognition of this rapid opiate analgesic effect has resulted in numerous research publications confirming its effectiveness. Studies investigating treatment of acute pain via opiate delivery across the nasal mucosa note equivalent or superior pain control to IV, IM and subcutaneous delivery methods.[3-6] In the post-operative setting, patient controlled intranasal analgesia (PCINA) systems used to deliver intranasal fentanyl or sufentanil result in equivalent pain control as IV PCA devices and superior pain control to customary ward-delivered pain medication.[7-11] Oncologists are beginning to recognize the advantage of this delivery site and have posted a web site protocol for intranasal fentanyl and sufentanil directed to patients suffering breakthrough cancer pain that is resistant to standard therapy.[7] (click here for link) The U.S. military is even investigating intranasal analgesics (ketamine) as an option for their soldiers to self treat the pain associated with battlefield injuries and possibly self-extract themselves from the situation.[12]
(click here for slides)Advantages of intranasal opiate medications :
Concerns regarding intranasal opiate medications:
Therapeutic threshold, side effect threshold:
A common problem with IN medication delivery is that the clinician fails to give an adequate dose of the drug because they are used to using intravenous (IV) medications and are afraid to give a higher dose of "IV" medication via the nose. For example, to treat a child for a painful condition one needs at least 1.5 to 2.0 times the IV dose of fentanyl intranasally to begin seeing an adequate therapeutic effect. This may appear as a seemingly huge dose to the clinician and they will give less. Failure to use adequate dosing will lead to inability to achieve a therapeutic threshold and the patient will not have adequate effect from the medication. To understand the reasoning behind administering such "high" doses one must consider several factors. The first is bioavailability. For oral medications we often give 10 to 100 times higher doses of a medication – because it takes that much to achieve adequate blood levels. For intranasal medications the doses are not as high, but they do need to be more than IV doses to achieve adequate serum levels of medication.
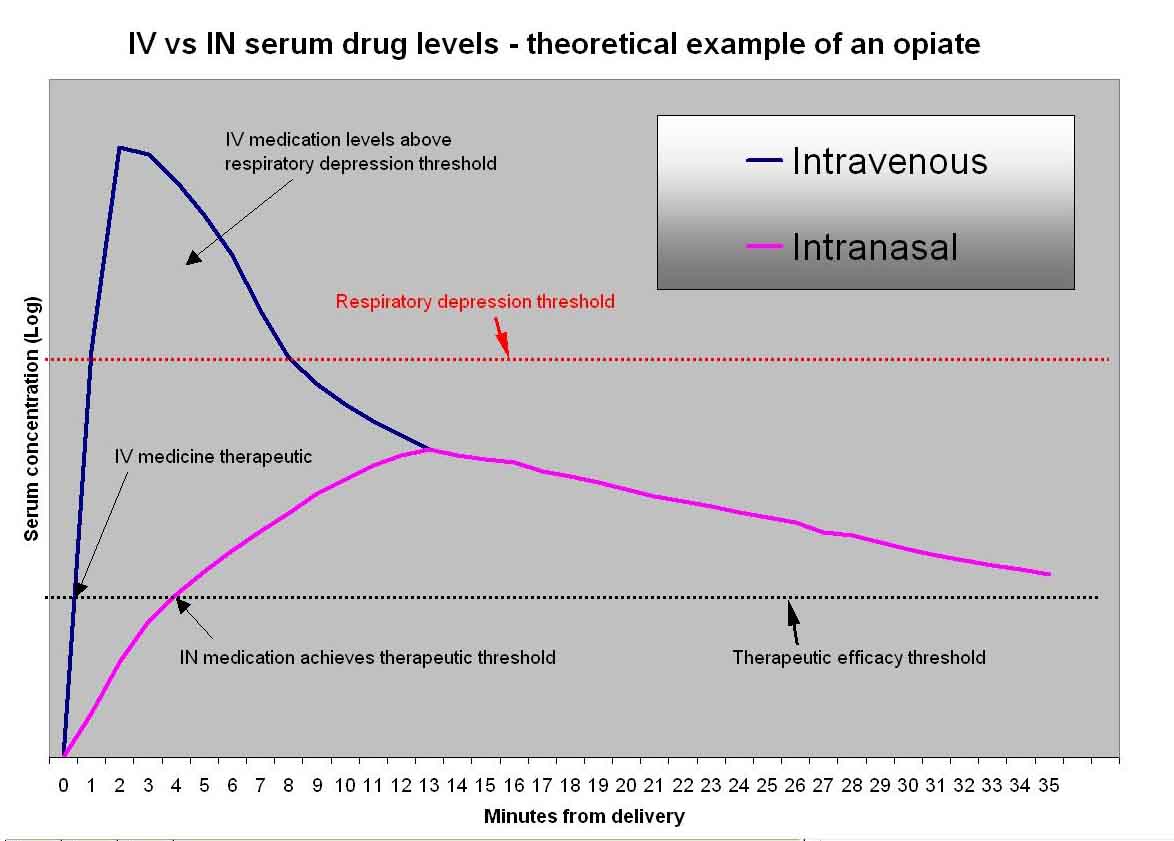
How much more will depend on the medication bioavailability. Secondly, the medication is not instantly in the serum when given via the IN route (as is the case with IV medication). It takes several minutes to absorb, often achieving therapeutic effect in 3-5 minutes and peaking at 10-30 minutes. Due to this delayed rise, IN medications given in proper doses will rarely achieve levels high enough to cause clinically important respiratory depression (the exception to this rule is when using sufentanil - it is so potent that inadvertent overdosing or administration to a patient who is already altered can result in respiratory depression and even apnea. For this reason be sure to give properly measured doses and to always monitor these patients). The following figure demonstrates a theoretical dose of intranasal versus intravenous opiate medication, demonstrating that the peak levels of the two methods of administration are far different, leading to less risk of respiratory depression when the IN dose is administered.
The exception to this concept occurs with the newer extremely concentrated synthetic intranasal opiates designed for hospice care. These drugs are concentrated to doses as high as several THOUSAND micrograms per ml (generic fentanyl is 50 mcg/ml). Using these very highly concentrated opiates on an opiate naive patient can lead to respiratory compromise and overdose due to the delayed but still very high levels of serum concentration achieved. A case report by Gracia in 2013 demonstrates this.[96]
Literature overview and discussion
Pediatric pre-operative and post-operative agitation/pain control:
Medications are frequently administered to children in the pre-operative setting to reduce separation anxiety and induce sedation. The most commonly used medications are benzodiazepines, however opiates or combinations of both are also frequently used. Numerous studies demonstrate that intranasal benzodiazepines and/or opiates are very effective for this indication.[22-28] Additional discussion of this literature can be found in the sedation section of this web-site. As a general summary of the literature, sufentanil seems to be the most frequently studied intranasal opiate used for sedation, demonstrating very effective sedation with reduced separation. However, the dosing regimens in the literature vary by a factor of 5, with the higher doses (over 2 micrograms per kg) leading to higher incidences of side effects such as respiratory depression, desaturation and prolonged sedation. Careful monitoring is suggested when this medication is used, especially in higher doses.
Myringotomy:
An additional group of studies have
specifically investigated the efficacy of intra-nasal fentanyl to
improve emergence characteristic of patients following myringotomy (a
procedure commonly done without an IV in place).[29,30,61,77,81,83,103,127] Both Finkel et
al and Galinkin et al found that intraoperative treatment with
intra-nasal fentanyl reduced post-operative agitation. Galinken also
noted a reduction in tachycardia, nausea, vomiting and recovery room
length of stay in-patient treated with IN fentanyl while Finkel found a
slight increase in PONV. Perhaps as
important, these two authors as well as a third (Voronov et al)
find that in children undergoing myringotomy (no IV at all) they were
able to easily control pain at the end of the case with intranasal
fentanyl. [29, 30, 61] In a more recent study Rampersad found IN
fentanyl equivalent fro controlling post-operative myringotomy pain to
other non-opioid medications, however these authors used a dose (1
mcg/kg) that is probably barely effective when given intranasally so one
would not expect much effect on pain.[77] Pestieau
compared IN fentanyl to IN
dexmedetomidine and placebo for post-operative myringotomy pain and
agitation. Both fentanyl and dexmedetomidine resulted in better pain
control than placebo. However, the study had to be stopped early due to
overly long sedation in the high dose dexmedetomidine group.[81] This is
not entirely surprising since the length of action of IN dexmedetomidine
is around 60-100 minutes. The authors conclude that IN fentanyl or
rectal acetaminophen are very effective and therefore the longer length
of time in recovery for IN dexmedetomidine cannot be clinically
justified in short operative cases such as myringotomy where the drug
effect is so prolonged.
Post-operative abdominal pain:
Heshmati et al found intranasal sufentanil (0.7 mcg/kg) effectively treated the pain of lower abdominal surgery within 10 minutes time in thirty children.[48] They noted only two episodes of nausea and no respiratory compromise, excess sedation, hemodynamic effects or desaturation. They conclude that intranasal sufentanil in this dose range is rapidly effective and safe and suggest that it be considered not only in post-operative care but also as a triage initiated pain medication in the emergency department. Additional investigations note IN opiates are appropriate alternatives for pain treatment in the post-operative pediatric patient.[31, 32]
In a recent review of the drug Sufentanil, Lundeberg and Roelofse tout their experience with over 1000 uses of intranasal sufentanil in pediatric anesthesia practice.[74] Here is what they say:
"At Astrid Lindgren Children’s Hospital, Stockholm, Sweden we have used intranasal sufentanil for reducing procedural pain, and infrequently as premedication for more than a decade, and in over 1000 patients. Our clinical experience is that the dose of sufentanil could substantially be decreased when changing the mode of application from drops to an aerosol. The onset is also faster with the aerosol.
Different devices could be used for creating an aerosol but we favor ...atomization devices, for simplicity and accuracy of dosing. The onset of sufentanil aerosol is about 5–10 min with a maximum sedative and analgesic effect at about 20– 25 min. Depending on the dose used, the effect wears off at about 60 min. Doses used for procedural pain are usually 0.7–1
ug/kg) and very occasionally over 1.5 ug/kg). These doses (<1.5 ug/kg) very seldom give adverse effects like nausea ⁄ vomiting and ventilatory depression. Lower doses of intranasal sufentanil can be used when combined with other drugs such as intranasal s-ketamine or dexmedetomidine."Other post-operative pain situations:
Yenigun et al showed that either IN fentanyl or IN ketamine were effective analgesics for children following tonsillectomy.[146]
Adult Postoperative pain control:
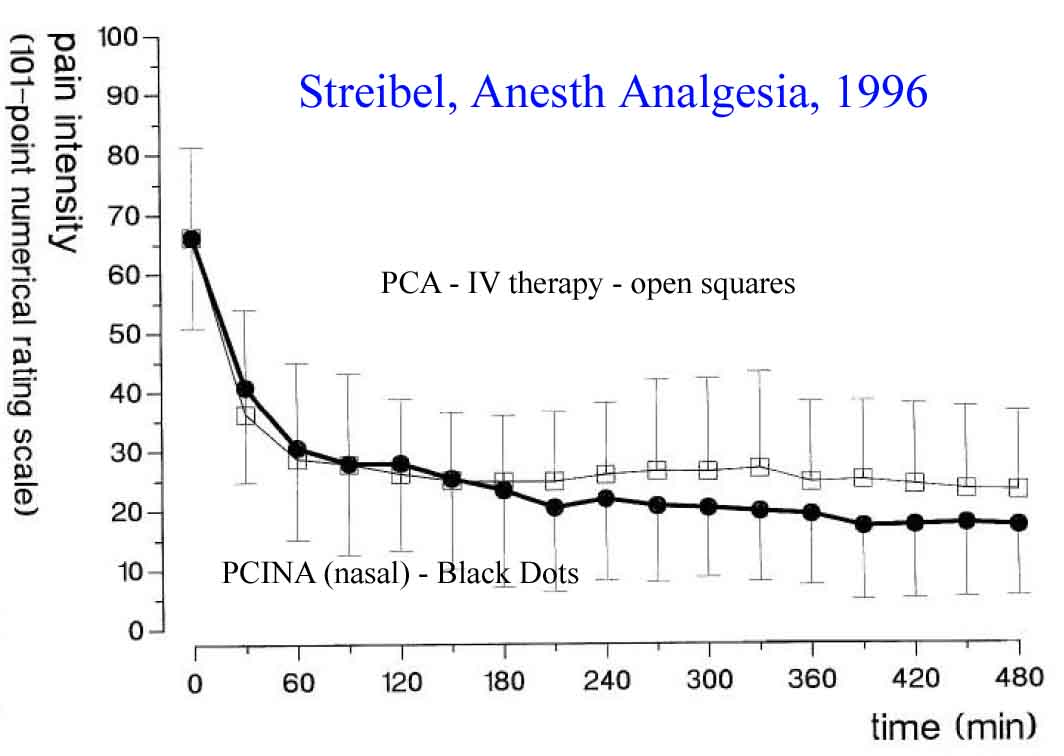
Striebel is the thought leader in adult post-operative pain therapy using intranasal opiates. He and his colleagues have published multiple studies investigating both nurse administered as well as patient administered intranasal fentanyl or intranasal meperidine (pethidine) in patients following surgical procedures.[3, 4, 8-10, 33, 34] These investigators used non-concentrated IV formulations of the opiate medication and overcame the volume issue by administering multiple small doses in a titrated fashion. In all of this groups published data the intranasal formulation was equivalent in onset of action and quality of pain control to the IV delivery route. Furthermore, when the patient was given control of dosing using a patient-controlled intranasal analgesia pump (PCINA) there was improved satisfaction and improved pain control due to the lack of need for a health care worker to respond to the patients pain needs.
Christrup et al confirmed Striebel’s data in a double blind, crossover trail in patients undergoing multiple molar extractions. They found the IN and IV fentanyl were equivalent in quality of pain control and in duration of effect.[35] Other authors have found similar results using various different opiate formulations.[36-39]
Hallett et al noted that intranasal diamorphine (heroin) provided good to complete post-operative pain relief in the majority of patients studied, but the delivery system they used suffered some technical problems, leading the authors to conclude that the concept is valid but the delivery system needed improvement.[40]
Abboud et al noted that intranasal butorphanol was superior to placebo, but of slower onset than IV butorphanol in treating post-cesarean section pain.[41]
Cannon found adequate pain relief with IN butorphanol in about 70% of his post-op head and neck outpatients.[42] A review of additional data on intranasal butorphanol can be found in an article by Gillis and a review by Dale.[18, 43]
Stoker et al compared a modified and concentrated form of intranasal morphine (generic morphine is not lipophilic and does not absorb well so needs to be modified for adequate nasal absorption) to intravenous morphine for treatment of postoperative bunionectomy pain.[38] These authors confirmed others findings that intranasal opiates are equivalent to intravenous opiates in terms of pain control.
Han published an interesting article noting that low doses of intranasal sufentanil if effective at reducing myoclonus seen during etomidate induction (click here for link to abstract).[56] Sufentanil is 5 to 10 times as potent as fentanyl and is probably the opiate of choice for nasal delivery in adults with severe pain based on preliminary data discussed in this web site and in the hospice literature.
A trial by Nave in 2013 sought to define the
bioavailability and efficacy of nasal vs buccal fentanyl.[95] The
authors used 24 volunteers as their own controls and measured plasma
fentanyl levels following delivery of 100 mcg of fentanyl via the nasal
cavity or via buccal mucosa using an oral transmucosal fentanyl lozenge
(lollipop). At 15 minutes time, plasma levels of fentanyl were 602 vs 29
pg/ml. There were no significant side effects noted.
The conclusion – a single dose of nasal fentanyl provides
significantly higher plasma levels and bioavailability than the buccal
route.
Editorial
note: This is yet another of many trials both in the pain literature and
the epilepsy literature (many featured throughout this web site)
demonstrating faster onset of therapeutic levels and higher
bioavailability of drug when given via the nasal mucosa as opposed to
via the buccal mucosa. It seems apparent that if time of onset and
patient compliance are an issue – the nasal routes is preferred.
Miscellaneous inpatient uses of nasal pain medications.
Child Birth
Fleet conducted an RCT comparing IN and SC fentanyl to IM
pethidine (meperidine, Demerol) in women in labor. They found pain
control to be similar, but the IM pethidine group mothers and babies
were frequently over sedated, labor was prolonged, and patients were far
less satisfied.[112]
Intranasal ketorolac (Toradol)
Moodie et al note that intranasal ketorolac (30 mg)given postoperatively results in reduced need for opiate rescue medication, less tachycardia and fewer fevers.[58] It was well tolerated and might be considered as a method of ketorolac delivery in appropriate clinical situations. Other authors confirm the effectiveness of IN ketorolac.[110] It is now available as a prescription prepackaged drug.
Acute pain in the Emergency department and prehospital setting:
Several well designed randomized controlled trials exist that demonstrate intranasal opiates are clinically equivalent to intravenous morphine and superior to intramuscular morphine for the management of acutely painful conditions in children.
Intranasal opiates (fentanyl , diamorphine, sufentanil, ketamine) for acute pain in pediatric and adult emergencies:
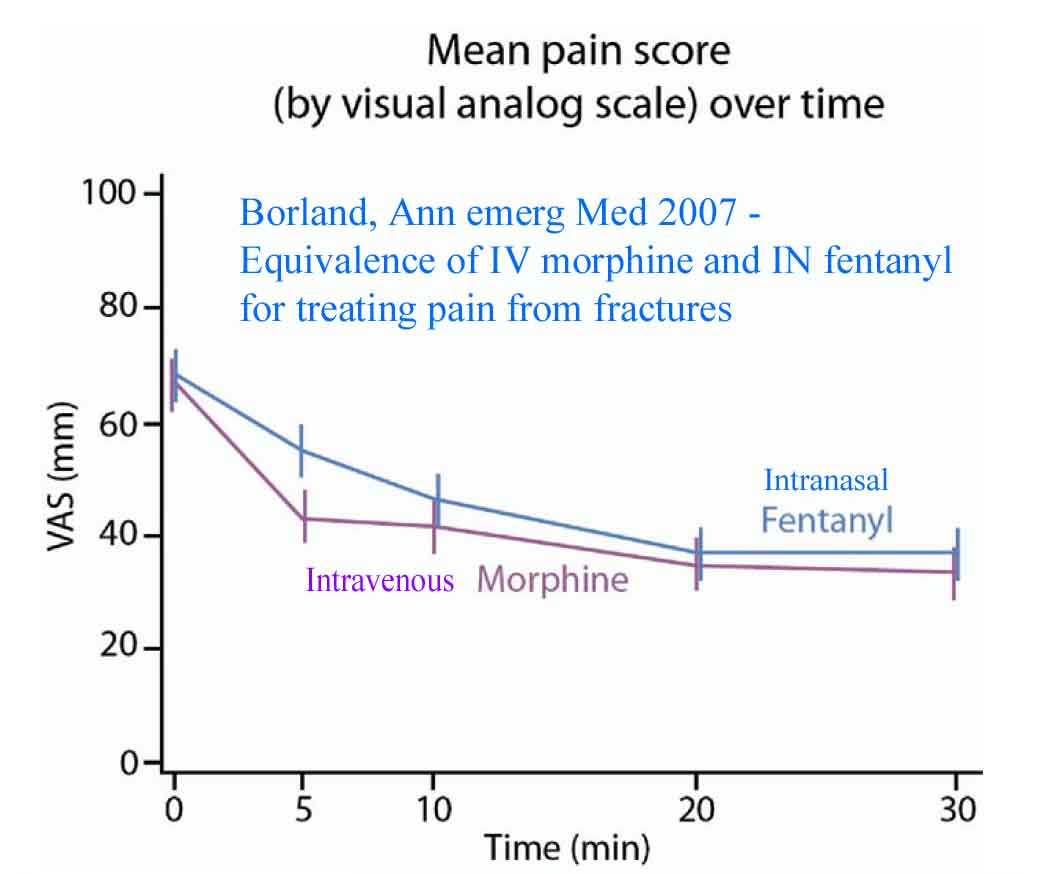
Borland et al conducted a randomized, double blind placebo controlled trial comparing atomized intranasal fentanyl (mean dose 1.7 microgram/kg) to intravenous morphine (mean dose .11 mg/kg) in children with acute pain due to long bone fractures.[13] 67 patients were randomized. Visual analog pain scores demonstrated clinically significant reductions in pain scores by 5 minutes that persisted throughout the entire study (out to 30 minutes) for both IN fentanyl and IV morphine (see diagram). Pain score reductions were equivalent for both study drugs. The authors point out that time delays were required to start an IV in the children before they could receive the study drug – a delay that could be eliminated if IN fentanyl were used in a non-blinded fashion. Given the clinical equivalency of these two modalities they conclude that IN fentanyl offers the advantage of a noninvasive, simple painless method for treating acute pain. These advantages suggest that this therapy would be useful not only in the emergency room but also in an EMS setting and at triage to allow more rapid onset of pain control in children suffering severely painful conditions. It could also be used prior to IV establishment, allowing time for topical anesthetics to take effect on the skin.
In a follow-up study to her randomized trial, Borland et al report on the results of clinical experience once IN fentanyl was introduced as a standard treatment in their pediatric emergency room.[50] She found the average time from triage to administration of opiate medications (Intranasal fentanyl versus IV morphine) dropped from 57 minutes prior to introduction of intranasal fentanyl, to 24 minutes following introduction. Furthermore, the eventual need for an IV to give further pain control in these cases was reduced from 100% to 42%. This real world observational report confirms the ability to speed up delivery of care while reducing resource utilization when intranasal medications are implemented for appropriate situations.
In 2011 Dr. Borland and colleagues published additional data regarding atomized intranasal fentanyl - a randomized controlled trial comparing generic 50 mcg/ml fentanyl to more expensive custom concentrated fentanyl (300 mcg/ml) in children (age 3-15 years) with painful extremity fractures.[79] There was substantial improvement in pain at 10, 20 and 30 minutes for both concentrations and there was no statistical difference (or clinical difference) in the reduction in pain scores. More of the heavier children (> 50 kg) required additional acetaminophen or NSAIDS at some point in their care. This data supports the use of inexpensive generic fentanyl for treating painful fractures in children. (Editor note - if you need more concentrated opioids for IN delivery in adults or opioid tolerant patients, sufentanil is also generic and is about 5-8 times more potent than fentanyl - in essence providing you a non-customized readily available opioid for nasal delivery)
Saunders et al conducted a similar trial assessing the efficacy of 2 mcg/kg of IN generic fentanyl (50 mcg/ml) in pain reductions for pediatric orthopedic trauma. They found effective control and high satisfaction scores using this treatment method.[44]
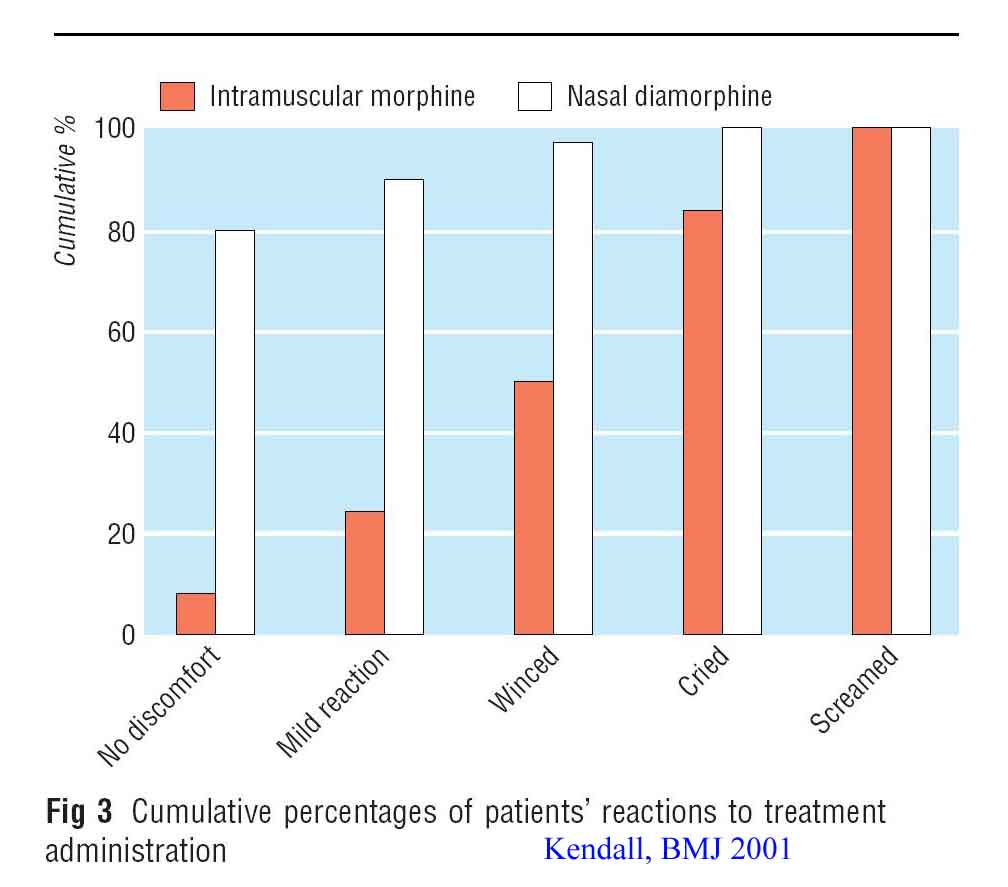
Kendall et al conducted a randomized controlled trail comparing intranasal diamorphine to intramuscular morphine in 404 children and teenagers with extremity fractures.[6] Intranasal therapy provided superior pain control at 5, 10 and 20 minutes while pain control was similar for both study groups by 30 minutes. Treatment acceptability as judged by nurses and parents was 98% and 97% for intranasal therapy versus 32% and 72% for intramuscular therapy (see diagram above demonstrating patients reactions to each ty
pe of therapy). The authors conclude: "Nasal diamorphine spray should be the preferred method of pain relief in children and teenagers presenting to emergency departments in acute pain with clinical fractures. The diamorphine spray should be used in place of intramuscular morphine."A few years later this same author (Kendall) conducted a pharmaceutical safety trial of diamorphine 0.1 mg/kg in children, specifically looking for adverse events. They entered 226 patients with acute pain and found a 26% incidence of mild side effects consisting of nasal irritation. There were no episodes of respiratory depression and 3 episodes of sedation (reduction in GCS). They conclude that despite some expected side effects, there were no safety concerns.[102]
Cole investigated the efficacy of intranasal fentanyl (50 mcg/ml) in children ages 12 to 36 months who were suffering painful injuries in need of more than an oral medication.[62] In a prospective sample of 57 patients these authors found a mean initial pain score of 8/10 with pain reduction to a mean of 2/10 by 10 minutes (93% had control of their pain) and to a mean of 0/10 by 30 minutes (98% had control of their pain). There were no complications and the delivery was well tolerated (nasal fentanyl does not burn nor taste bad). They conclude this is an effective, safe, well-tolerated method of pain control for moderate to severe pain.
Holdgate evaluated the time it took to treat children (ages 1-15 years) with acute pain when IV morphine was the standard, compared to after the introduction of intranasal fentanyl.[63] The study occurred in a mixed setting ED (adult and pediatric emergency department). In the 7 months before study implementation they administered opiates (IV morphine) to 63 children. In the 7 months after study implementation they provided opiates to twice as many children (118 patients). 81 children received intranasal fentanyl while 37 received IV morphine. The median time for delivery of pain control was 32 minutes for nasal fentanyl and 63 minutes for IV morphine. Furthermore, there was a clear trend to provide opiates via the nasal route to younger children (who might otherwise NOT get pain medicine due to the need for an IV). Median age for IN fentanyl was 8.5 years while it was 12 years for IV morphine. The authors conclude - "This study demonstrates that children treated with IN fentanyl received analgesic medication faster than those treated with IV morphine in a mixed ED. Younger children were more likely to receive opioid analgesia following the introduction of fentanyl."
Schacherer et al further confirm that an IN fentanyl
pathway results in a significant decrease in time to pain medication
administration for long bone fractures. In his study they decreased time
to pain medication delivery from 62 minutes (IV morphine) to 37 minutes
(IN fentanyl) with equivalent ability to control pain.
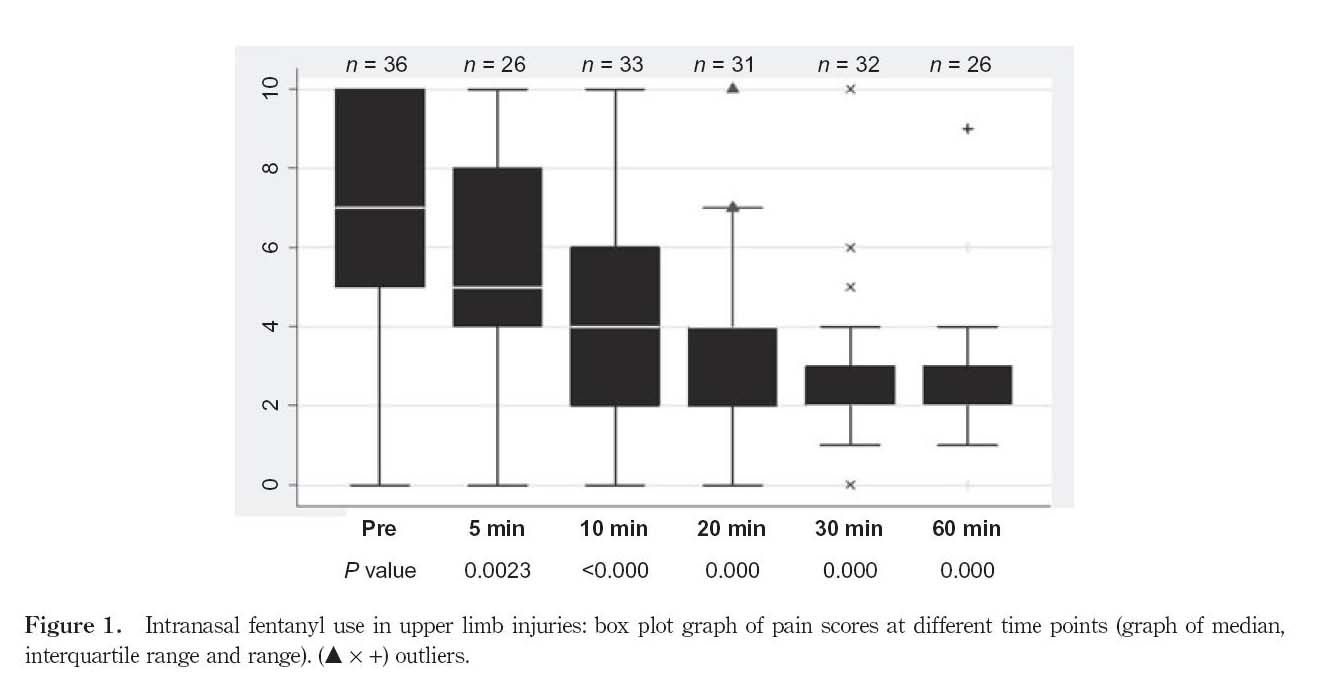
Crellin et al evaluated the efficacy of generic IV fentanyl (50 mcg/ml) for treating orthopedic pain in children 5-15 years of age.[64] They found it very effective with pain score reductions from 7 at onset to 5 in 5 minutes and 2 at 30 minutes (see above figure). Mean time from triage to drug delivery was only 20 minutes. They titrated to effect with multiple doses as needed. It was well tolerated and very inexpensive. The authors conclude that generic 50 mcg/ml fentanyl is very effective, well tolerated and inexpensive method for treating painful injuries in children.
Regan found intranasal diamorphine to be equivalent to
intravenous morphine in terms of time to administration of the drug in
children in his A&E department.[84] However, there was less frequent need
for further analgesia using the nasal medication. They conclude that
nasal diamorphine remains a preferred agent and note that it has been
adopted in 60% of U.K. emergency departments.
Adelgais et al retrospectively reviewed 5 years of data comparing IV
opiates to intranasal fentanyl using three Institute of Medicine quality
indicators (timeliness, safety and effectiveness). 1702 patient
encounters were reviewed. This study
is unique in that IN fentanyl
was used not just for orthopedic cases but was used for any
patient that needed opiates. They
found that patients receiving IN fentanyl had a shorter time to delivery
of pain medications, faster onset of analgesia (39 vs 68 minutes) faster
time to discharge from dosing (109 vs 203 minutes), shorter ED length of
stay (168 vs 267 minutes) and equal efficacy of pain control. This is
yet more data supporting prior studies showing that IN fentanyl is just
as good as IV opiates for controlling pain, but results in much faster
patient throughput time and less resource utilization.
Harlos et al have even used nasal fentanyl in newborn babies who are
suffering from terminal illnesses in an effort to reduce their pain and
suffering.[86] They demonstrated safety and efficacy (as well as
possible in this unique setting) and felt this was more compassionate
than an injection. Prior to this publication the youngest reported age
of nasal atomized fentanyl was 3 months old.
Sheier et al found that ketamine 1 mg/kg given 15 minutes prior to
difficult IV starts was very effective in reducing pain and anxiety in
both children and their parents.
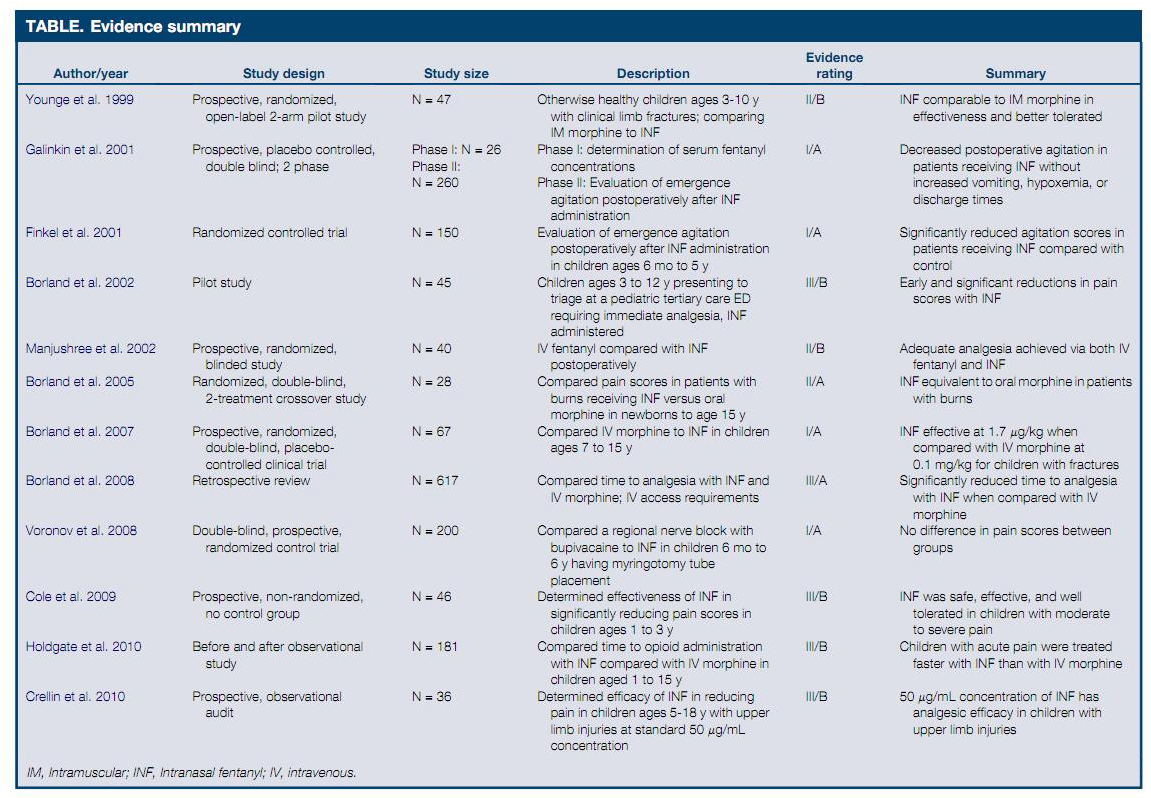
A nice review of most of these pediatric articles prior to 2011 was published in September 2011.[80] The conclusions are that IN fentanyl is equivalent or superior to morphine administered IV, IM or orally and that it is much faster in onset. Furthermore it is safe and does not require compounding (generic 50 ug/ml is fine for children). Given this efficacy, safety and low cost it offers an approach to improve care, improve satisfaction and reduce resource utilization.
Click here for a table from the article that summarizes all the articles.
{kind=link}
Interestingly a 2014 Cochran review on IN fentanyl use in children with acute pain is probably a good idea but concludes that the data is inadequate to draw many conclusions.[105]
Nielsen et al found that a combination IN sufentanil (0.5 mcg/kg) plus ketamine (0.5 mg/kg) was effective at preventing / reducing pain in 78% of children given this combination prior to a painful procedure.[106]
Graudins et al showed that IN ketamine at subdissociative doses (1 mg/kg intranasal) is equivalent to intranasal fentanyl (1.5 mcg/kg) for controlling acute moderate to severe pain in children with limb injuries.[117]
Tsze et al describe a Tetralogy of Fallot case where the baby was
suffering an acute hypercyanotic spell (oxygen sats 56%) that failed to
respond to knee chest positioning.[108] They successfully reversed the
episode using IN fentanyl.
These children are on a physiologic knife edge and if you frighten them
or hurt them they can decompensate severely (or die) with an increase in
their right to left shunting of blood in the heart. Traditional
treatment includes oxygen administration, knee-chest positioning,
calming the patient AND administering IV morphine. Obviously IV starts
in these situations are both difficult AND not calming to the child.
These authors are the first to publish data on using intranasal opiates
rather than IV opiates to calm the child – with no need for establishing
IV access in the midst of a dangerous hypercyanotic spell. This therapy
will never enter the realm of a randomized controlled trial due to the
infrequency of the event so these kinds of case reports are all we have
and can assist us in changing practice to better care for these complex
but rare conditions.
Fenster et al compared IN fentanyl (2 mcg/kg) to IV morphine (1 mg/kg) for
pain control during abscess incision and drainage.[124] They found pain
control and patient satisfaction was superior with IN fentanyl and
required less time and resource utilization.
Murphy et al conducted a prospective study evaluating the efficacy of IN
fentanyl to treat severe pain in children cared for by their prehospital
providers. They found clinically significant pain reductions in 83% of
children with a median pains score reduction from 10 to 5 in ten
minutes.[126] There were no adverse events associated with the
treatment. They conclude this is a safe and effective treatment and
maybe an attractive alternate to oral and IV opiates.
Quinn et al conducted a small but well designed study demonstrating what
most other similar studies have shown: That IN ketamine is a good pain
reliever for children with acute pain, though perhaps not quite as good
as IN fentanyl and with a higher side effect profile. It does provide a
reasonable an alternate to an opiate however.
Elitsur and colleagues (2019) utilized a minimal sedation and analgesia
protocol to reduce pain and anxiety in patient with juvenile idiopathic
arthritis who needed steroid injections in their joints. They were able
to combine several agents including intranasal fentanyl into a regimen
that resulted in pain scores of 1 for the patients. The result of this
protocol change was the reduction of the need for general anesthesia to
do this procedure and resultant dramatic drops in hospital charges –
(and probably in length of stay.)
Frey et al conducted a prospective randomized trial that compared the
efficacy of IN ketamine (1.5 mg/kg) to IN fentanyl (2 ug/kg) in children
with extremity injuries. They gave adequate doses of the medications
bases on prior research and found that the two treatment modalities
resulted in equivalent reductions in pain scores (about 3 out of 10).
There were slightly more minor adverse events (dizzy, drowsy, bad taste)
in the ketamine group but no serious adverse events.
Guthrie et al did a chart review to evaluate their staff impression and
patient outcomes when IN ketamine was used for analgesia or mild
anxiolysis/sedation. They found high provider satisfaction and a drop in
use of IV medications for analgesia and sedation. Interestingly (but not
surprising if you have been paying attention for the last decade and are
willing to use the proper does to obtain you clinical effect) the
doctors preferred ketamine in the 3-5 mg/kg dose – higher than we see in
many studies. Side effects occurred in 6% but were all minor (nausea,
dizziness, drowsiness).
Lord et al did a large data base review of pediatric EMS
transports and found that once IN fentanyl was introduced they noted a
significant increase in children who had clinically relevant reductions
in their pain scores during transport.
Miguez found that Orthopedic procedural sedation and pain control using IN
fentanyl and nitrous oxide was equally effective as IV ketamine with
fewer side effects and shorter lengths of stay.
Williams and colleagues reviewed their experience in a pediatric urgent
care and found that intranasal fentanyl and midazolam are safe and
effective in this less resource intense setting.
Ku conducted a small retrospective study on 17 neonatal ICU patients and
noted that IN midazolam and fentanyl were safe and effective in this
population.
Sindhur et al evaluated the safety and efficacy of IN fentanyl in 111 premature infants (2 mcg/kg – a well established effective dose) to assist them in assessing retinopathy of prematurity.[166] They found this treatment significantly reduced pain with NO evidence of respiratory depression.
Editorial comment:Here is data showing IN fentanyl is pretty darn safe. These authors gave this drug to 111 premature children at full dose and found NO issues with respiratory compromise.
Turner investigated IN Ketamine (0.1 to 0.2 mg/kg titrated to effect
using up to 5 doses) for treatment of migraine headaches in children,
finding it to reduce pain by 66%.[167] They suggest ketamine should be
added to your therapeutic options for
migraine treatment.
Intranasal opiates for acute pain in adults
Most of the emergency medicine literature relating to intranasal opiates
focuses on pediatric cases due to the desire to limit further pain from
starting an IV or giving an intramuscular injection. However, intranasal
opiates are also very useful in the adult patient (see the EMS and Burn
sections below). Many adults with minor acute burns, orthopedic trauma
and other painful conditions often get an IV line for
pain control (no resuscitation
needed). In this setting nasal opiates are very effective, save nursing
time and are well accepted by the patients.
Steenblik published a series of 40 patients with acute orthopedic trauma who were cared for in a ski clinic that confirms the above statement.[82 ] In this non-blinded clinical trial the investigators entered patients that they cared for in a ski clinic who were suffering from moderate to severe pain related to orthopedic trauma. The mean pain score on study entry was 9 (on a 10 point scale). Patient all were administered intranasal sufentanil (chosen rather than fentanyl due to higher potency and smaller weight based volume) at a does of 0.5 mcg/kg.
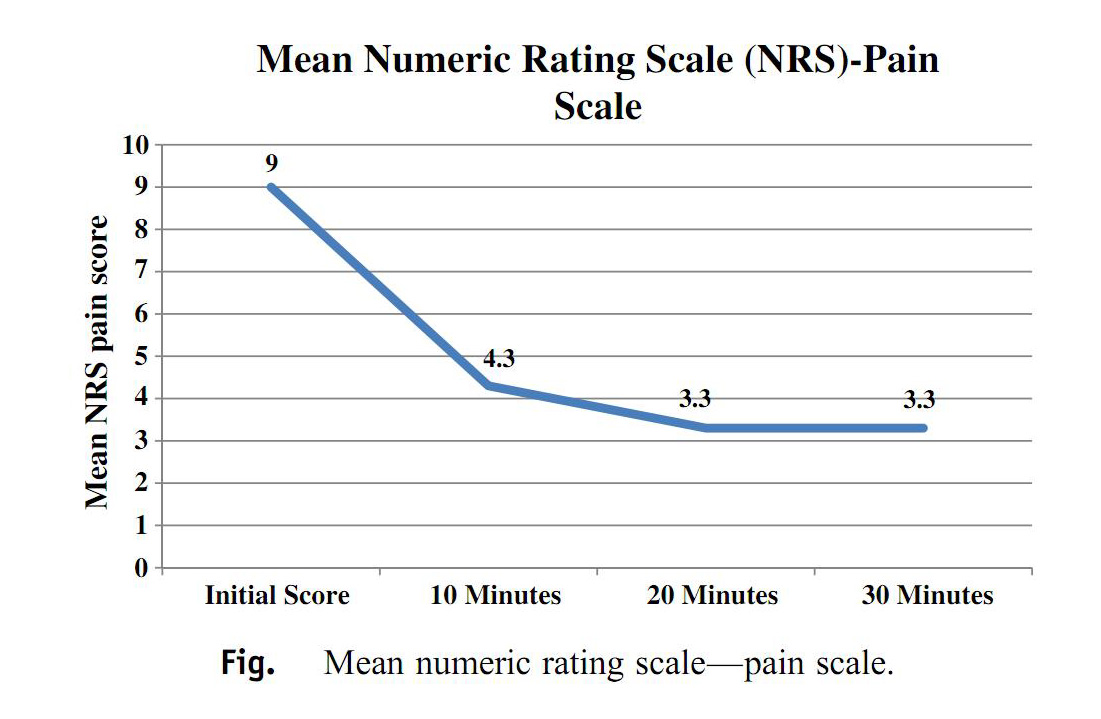
This treatment was successful in 95% f patients with a mean reduction in
pain from 9 to 4.3 at 10 minutes and 3.3 at 20 minutes – a highly
clinically significant reduction in pain.
On a 5 point satisfaction scoring they found that “very
satisfied” answer in 78% of patients, 83% of nurses and 87% of
physicians. There were minimal side effects – dizziness being the most
frequently reported. One patient dropped their saturations to less than
92% after a second dose of nasal sufentanil was given due to inadequate
pain control. The authors conclude that intranasal sufentanil provides
rapid and adequate pain control in austere conditions and can be easily
administered with no pain to the patient.
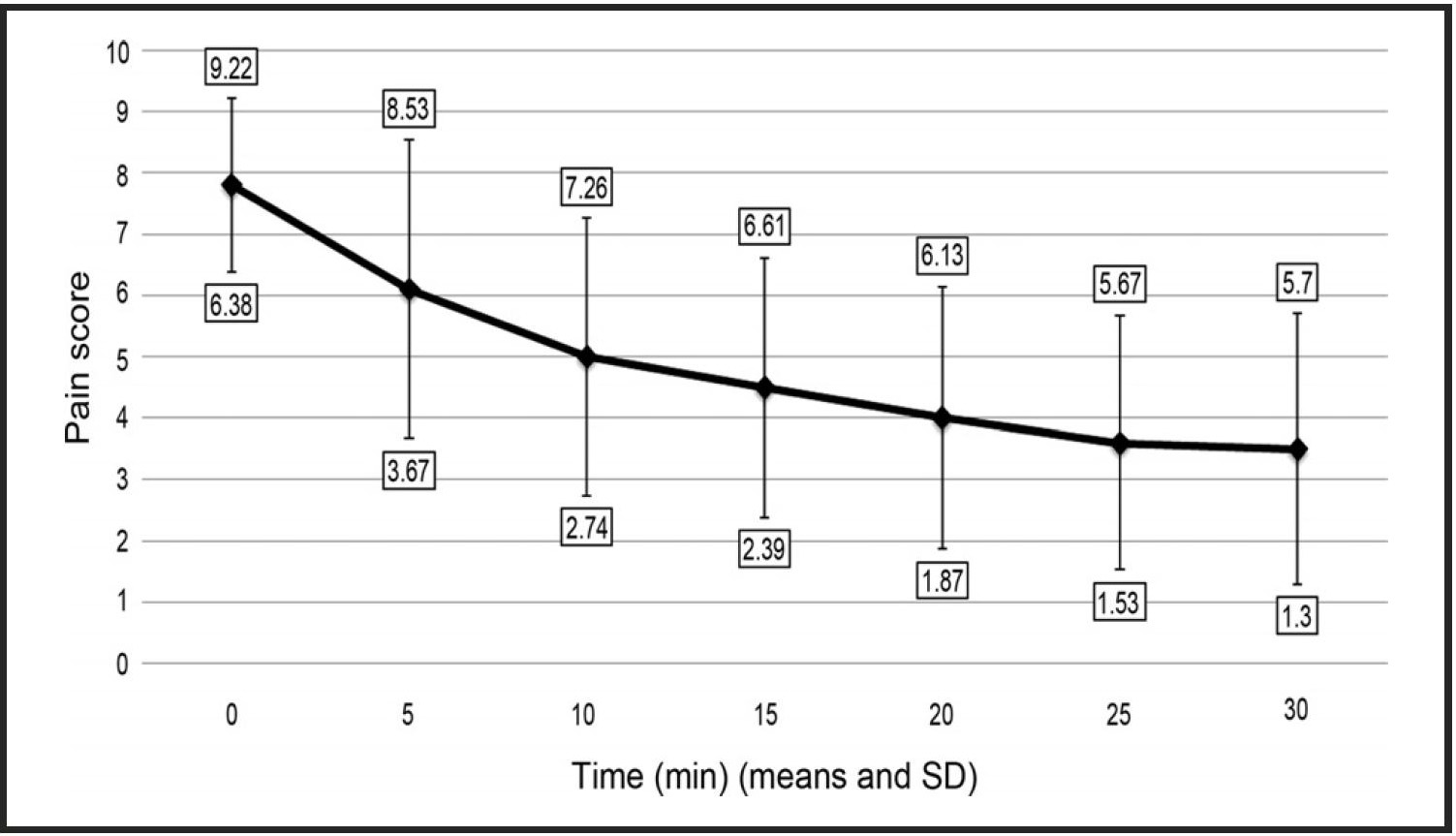
Stephen investigated the efficacy, safety and satisfaction scores when IN sufentanil was used in adults with acute orthopedic trauma.[85] Using a dose of 0.5 micrograms per kg they found pain scores dropped from 7.8 to 3.5 within 30 minutes, that of the 15 patients studies only one had a reduction in their pulse oximetry below 90% (88%) but 46% had some sensation of feeling whoozy. Satisfaction scores for patients, nurses and physicians (5 Point Likert score with 5 being the best) were 4.5, 4.0 and 4.2 respectively.
The authors conclude this is an effective, safe
method to treat acute pain in adults and sufentanil offers many highly
desirable features (volume of administration, potency, therapeutic
index, cost) for use in the emergency setting.
Dolatabadi et al conducted a randomized controlled
trial directly comparing IN sufentanil (0.3 mcg/kg) to intravenous
morphine ( 0.1 mg/kg - gold standard) for severe pain related to
extremity trauma in 88 adult patients.[116]
Both therapies provided equivalent pain control with no
difference in time to onset after drug delivery. Side effect profiles
were similar. They conclude that IN sufentanil is equivalent to IV
morphine for quality of pain control and is rapid, efficient and
non-invasive.
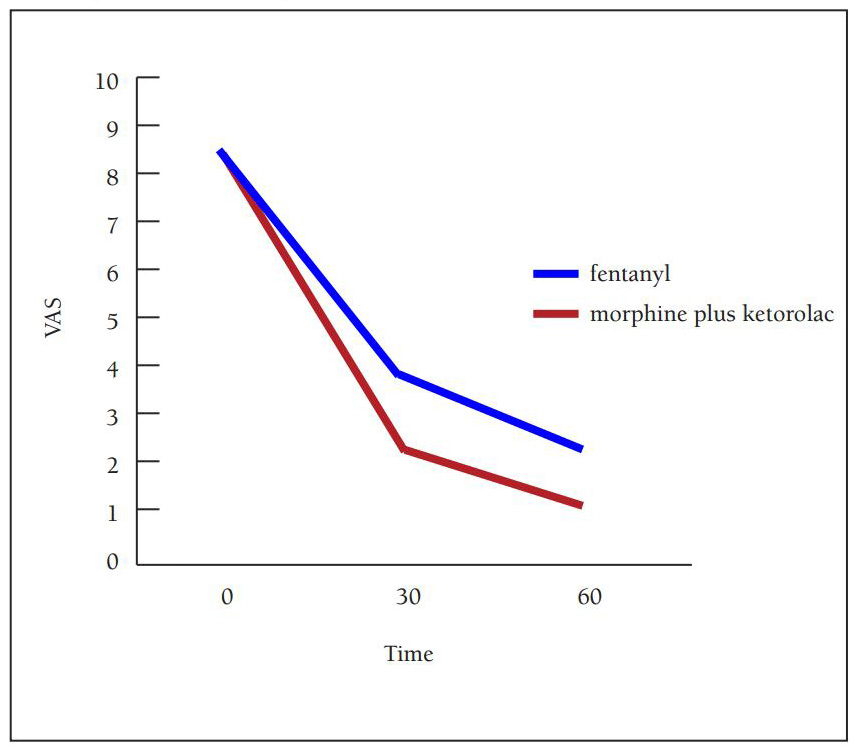
Etteri et al did a very nice clinical trial that
compared IV morphine plus IV ketorolac (5 mg / 30 mg) to intranasal
fentanyl (3 mcg/kg of 50 mcg/ml solution) for the treatment of acute
renal colic in adults. Not surprisingly, the IV formulation was superior
in efficacy. However, it is still quite impressive how the nasal group
faired in terms of pain control for such an uncomfortable condition (see
the graph). Pain scores on a 10 cm VAS at entry, 30 minute and 60
minutes for the morphine/ketorolac IV arm were 8.6 / 2.3 / 1.1
respectively. For the intranasal fentanyl arm they were 8.8 /4.0 / 2.2
respectively. The authors conclude that for a condition as painful as
renal colic, IV morphine and ketorolac is the first choice of therapy,
while nasal fentanyl might be appropriate in a less controlled setting
such as out of hospital or nurse initiated setting.
Click here for the journals link to the article (free)
Editorial
comment: It is not surprising that the IV combination of an opiate plus
a NSAID worked better than an opiate alone for 2 reasons. First generic
concentrations of fentanyl tend to be a little less effective in adults
due to volume issues and second because non-steroidal anti-inflammatories
are a mainstay for successful therapy of renal colic. They are in
reality the best treatment over time, but take longer to work so we tend
to add an opiate to get pain more rapidly in control. I wonder if a
combination of concentrated fentanyl or generic sufentanil PLUS an oral
or nasal NSAID might not have changed these results. I have no research
data to support this opinion but do have personal experience (nasal
sufentanil plus oral ibuprofen) suggesting it is very effective. Future
investigators should strongly consider these minor protocol changes –
the authors actually admit the lack of a NSAID is a limitation to their
study design. I do agree
with the investigators that IV therapy is preferred if possible because
these patients frequently need multiple doses of drugs and nausea
medications and repeat evaluations, need their blood drawn to evaluate
renal function (so get a needle stick anyhow), etc. Never the less this
is a great study and helps us define the niche (or lack of niche) for
nasal drugs in our daily practice.
Belkouch et al conducted a prospective study
evaluating the efficacy of generic atomized intranasal fentanyl (1.5
mcg/kg, 50 mcg/ml concentration) for therapy of acute renal colic in
adult patients.[115] The patients who did not experience a significant
drop in pain by 5 minutes got rescue IV morphine for pain. 23 patients
were enrolled. VAS pain scores dropped significantly at all times
measures dropping from 85/100 at time zero to 48 (5 min) 35 (15 min) and
8 (30 min) - see graph (power calculations were not provided).
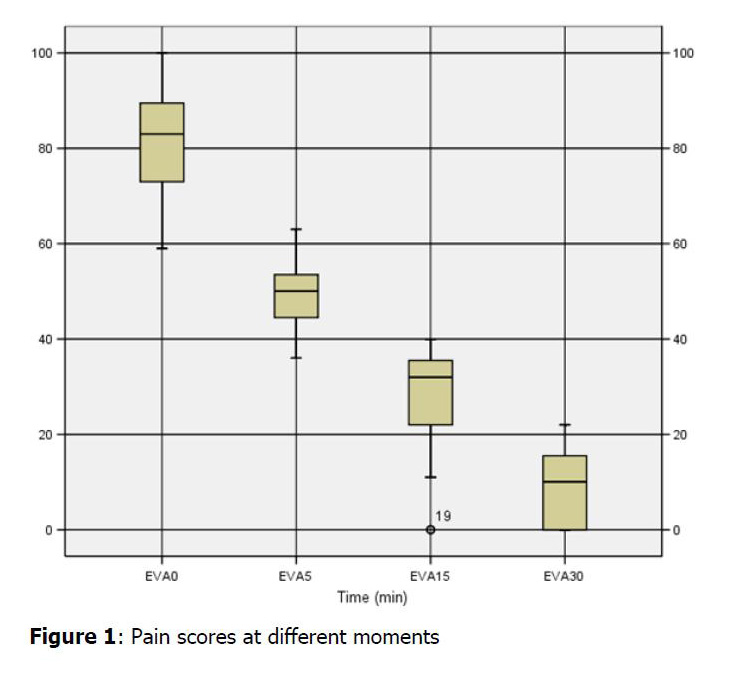
Graph comparing pain score versus time from Belkouch study
There were no adverse events. The authors feel that IN
fentanyl at generic concentrations (50 mcg/ml) is very effective, safe,
readily available, inexpensive and easily delivered. They conclude that
when compared to current practice (IV meds), IN fentanyl “has the
potential to improve patient and family satisfaction and could have
further implications related to improved cost-effectiveness and quality
of care.” This article
provides a possible inexpensive method of treating renal colic deserving
of more research: IN opiate,
IN ketorolac, transmucosal antiemetic, No IV started at all (IV fluids
do NOT assist in stone expulsion or pain control).
Chew et al showed that
adding IN fentanyl (1.5 mcg/kg) to IV tramadol improved pain scores in
adults with acute musculoskeletal injury when compared to IV tramadol
alone (drop of 29 vs. 19 points on a VAS).[123] They also noted a
transient but statistically significant drop in blood pressure (13.35
vs. 7.65 mm Hg less) though it is unclear whether that is a clinically
important drop (BP drop might be due to improved pain).
Kerr et al investigated titrated patient controlled
intranasal fentanyl for treating pain during child birth.[118] 32 women
were studied using a nasal PCA device that delivered 50 mcg of fentanyl
every 3 minutes as needed. The average titrated dose over 3.5 hours was
734 mcg. 78% of patients reported satisfactory to excellent pain control
and 85% said they would use it again. Perhaps not surprising, when
accumulated dosing exceeded 700 mcg there was some neonatal respiratory
depression requiring transient bag ventilation (12.5% of births).
Fleet et al also noted that birthing women prefer IN fentanyl that they
self administer for pain to either IM meperidine or subcutaneous
fentanyl.
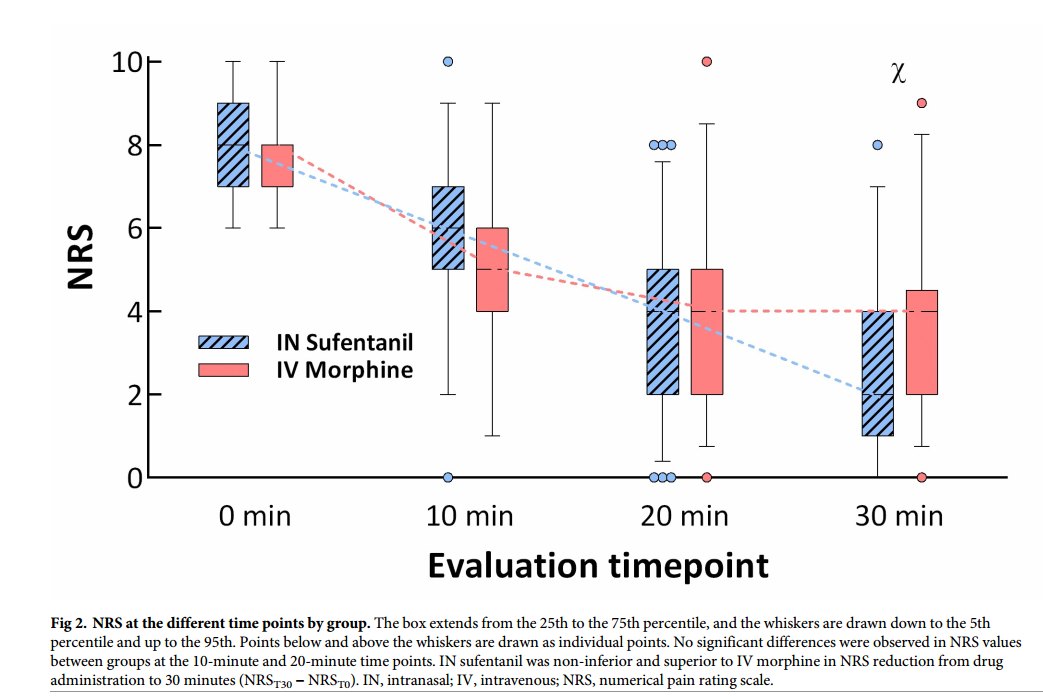
Blancher et al published one of several 2019 prospective randomized
trials comparing IV morphine to intranasal sufentanil in adults with
moderate to severe pain. They included trauma patients with pain scores
> 6 on a 10 point scale. This study differs from the study by Sin, et
al, (also 2019) in that it was done in Europe, it was multicenter and it
allowed titration of the medications to effective pain control levels.
They found sufentanil to be slightly superior to IV morphine for pain
control by 30 minutes (equivalent at 10 and 20 minutes), (though because
titration was allowed it seems they simply needed to give more
medication should they want lower pain scores.)
They also found a few minor incidences of hypoxemia in both
groups but more in the sufentanil group (3 of 67 versus 1 of 69). They
conclude that titrating sufentanil via the IN route allows early, safe
and effective analgesia in emergency settings and difficult situations.
Graph from
Blancher et al showing the reduction in pain scores (NRS – numerical
pain reduction score) for IV morphine and IN sufentanil in patients
suffering severe pain due to traumatic injuries.
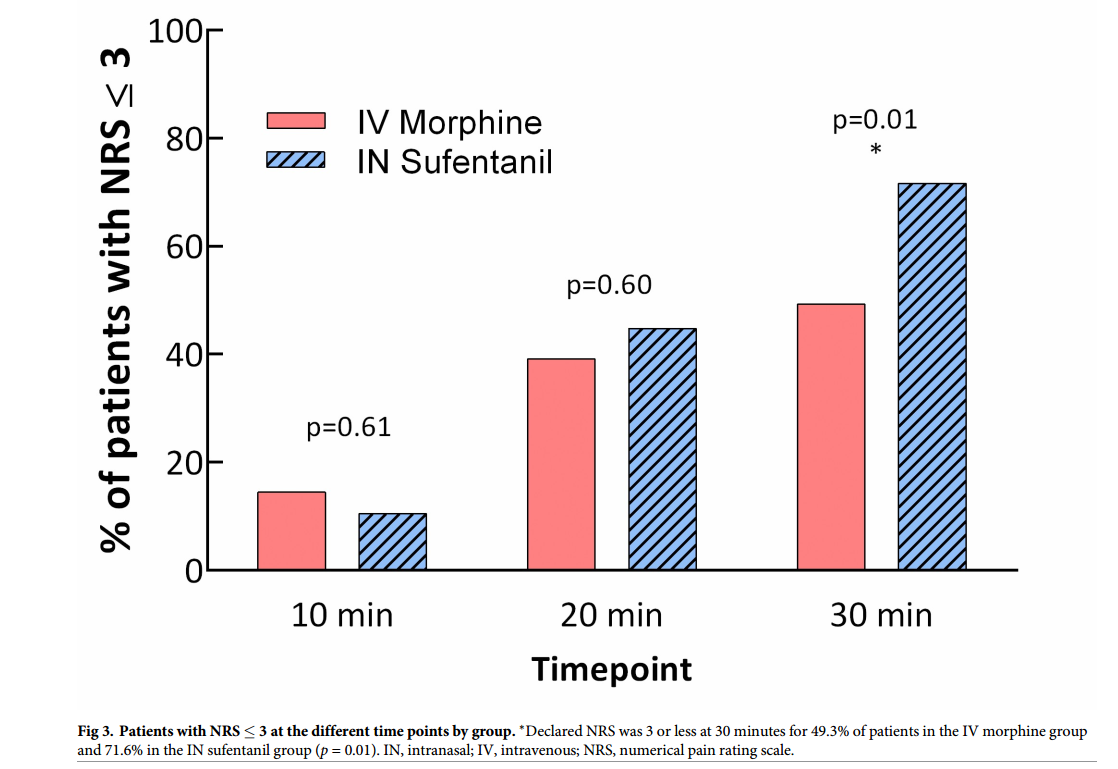
Graph from
Blancher et al showing the percentage of patients over time for whom
their pain scores become less than 3 on the pain scale. This study
allowed titration of IV morphine or IN sufentanil in patients suffering
severe pain due to traumatic injuries. The key point being that you can
easily and safely titrate pain to whatever level you desire using IN
sufentanil.
Lemoel randomized 144 patients suffering severe traumatic limb pain (>6/10)
to two cohorts: One got IN sufentanil in triage plus IV multimodal
analgesia as needed, the second got only IV multimodal analgesia.
Pain control and patient satisfaction
were the same by ED discharge, however the IN sufentanil group
had far high pain control (pain less than3/10) at 30 minutes from
arrival than the IV group:
72% versus 52%. One patient in each group required supplemental oxygen.
Mozafari found that a somewhat low dose of nasal ketamine of 1 mg/kg (given
the pain severity) effectively reduced pain associated with renal colic
from a mean score of 8.7 down to 2.5 in 30 minutes. This was slightly
less effective than IV fentanyl (9.7 to 1.3) but did not require an IV.
Nejati et al noted that intranasal ketamine at a single 50 mg dose in
adults effectively reduces pain associated with digital nerve blocks.
Sin et al conducted a prospective randomized trial compared IV morphine
to IN sufentanil in adults with moderate to severe pain. They found that
the two therapies were equivalent (pain scores decreasing from 9/10 to
2/10 for morphine and from
10/10 to 2/10 for sufentanil in 5 minutes.) There were infrequent
adverse events with none being serious.
Nazemian found that renal colic patients treated with IV fentanyl or IN
fentanyl (plus IM ketorolac in both groups) had identical significant
reductions in pain.
Emergency room throughput - can it be influenced by implementing
intranasal pain medications?
Intranasal opiates for ambulance patients:
Rickard et al conducted a randomized controlled trial comparing intranasal fentanyl to intravenous morphine in a pre-hospital ambulance setting.[16] 227 adult patients with severe pain (mean VAS score 8/10) were randomized to treatment, with pain scores repeated upon hospital arrival. Both methods were clinically equivalent with mean pain scores dropping to 4/10 by hospital arrival. The authors conclude that IN fentanyl is an effective alternate to IV morphine and is particularity valuable in situations where IV cannulation is difficult, unwanted or unnecessary. Other studies comparing intranasal opiates to alternate therapies for acute pain, have routinely found IN therapy to be an effective and acceptable route in the right clinical situation.[5, 14, 20, 21, 44]
McLean studied IN fentanyl (50 mcg/ml) in adult trauma patients seen at a ski clinic.[65] They treated 46 patients, using a mean does of 1.4 mcg/kg and found clinically significant decreases in pain scores by 2 minutes (14 mm VAS decrease), 5 minutes (28 mm VAS decrease) and 10 minutes (28 mm VAS decrease). they conclude this is an effective analgesic in acutely injured adults in whom immediate IV access is complicated by scenario or resource limitations. and feel its potential in search-and-rescue and other austere medical situations is widespread. (Web site Editors note - this is a relatively low dose of medication using a fairly dilute form for adults - yet it was still fairly effective and very inexpensive and safe.) (click here for abstract)
Johnston studied the efficacy of intranasal fentanyl given to over 500 adult ambulance patients for the treatment of non-orthopedic visceral pain (i.e. chest and abdominal pain). They found it effective with a mean pain score reduction of 32 mm on visual analog score.[67]
Middleton did a retrospective analysis of several thousand uses of intranasal fentanyl for acute pain in an ambulance setting.[75] They found it was about 80% effective at reducing pain by >30% during transport – perhaps very slightly less effective than IV morphine (81.8% effective) but that that benefit was likely offset by the need for an IV to deliver the morphine.
Bendall published another article of many noting that IN fentanyl is just as good as IV morphine for controlling acute pain in children.[76] The authors were allowed to titrate IV and IN drugs to effect allowing customization to the patients needs. The unique feature of this article is the clinical setting of EMS where IV lines in children are even more difficult and time consuming due to a variety of factors. The authors appropriately conclude that in light of the non-invasive route of administration and equivalence to IV morphine, IN fentanyl is the most suitable analgesic agent for managing pediatric patients with moderate to severe pain in the EMS setting.
Ellerton et al describe their mountain rescue
experience with opioid drugs for severe pain.[99] They found intravenous
opioids most effective (pain score down from 8 to 2) but also most
difficult to deliver. Intranasal diamorphine at 5 mg doses, titrate at
15 minutes was found to decrease pain scores from 8 to 4.5 by time of
handoff. They felt they needed to further address the proper dose (this
is a low dose unless they are treating small adults – more typically we
give 0.1 mg/kg) and determine if the cold environment impacted efficacy
and if adjusted for could lead to even more effective pain control.
Karlsen prospectively collected data to evaluate
the efficacy of IN fentanyl for severe pain in the prehospital
setting.[104] A total of 903 adults and children ages 8 or older with
severe pain due to orthopedic conditions, abdominal pain or acute
coronary syndrome refractory to nitroglycerin were evaluated. The
patients received 1-3 doses of IN fentanyl (either 50 or 100 mcg per
dose - range 50 to 300 mcg – of highly concentrated fentanyl ) titrated
to effect. 7% of cases were less than 18 years old, the remaining 93%
were adults. There were no serious adverse events, no respiratory
depression and no use of naloxone. Mild adverse reactions (nausea,
vomiting, vertigo, mild hypotension) occurred in 4%.
The
median initial pain score was 8 and the median pain reduction was 3
points on a 10 point scale.
Editorial comment:
Here is further evidence, in the largest EMS trial published to date,
demonstrating both the effectiveness and safety of IN fentanyl for
severe acute pain in ambulance patients. The authors demonstrate a high
level of understanding of this delivery technique by allowing titration
of the drug to effect, a concept that should be mimicked by further
researchers. Intranasal medication delivery for painful conditions
should be titrated just as IV medications are titrated – the right dose
is enough to have clinical effect without significant side effects. They
also chose a highly concentrated fentanyl (500-1000 mcg/ml) but data
from other studies have demonstrated that this is not required – generic
concentrations are adequate and effective especially when titrated.
Another promising concept for prehospital pain control is intranasal ketamine. Ketamine in sub-anesthetic doses (about 10-15 times less than doses used for deep sedation) is an excellent pain killer, yet does not cause dysphoria nor respiratory depression (see details below and in the hospice section). This lack of respiratory depression may make this drug an attractive acute pain treatment modality for both ALS and BLS providers (it is already being used by lay people in the military and hospice setting). Reid et al have published the first report of such use in the EMS setting.[78] They treated a 9 y.o. child who was burned with 0.5 mg/kg (or less due to dead space losses) and within 3 minutes the child's pain and anxiety resolved, he was able to assist in his transfer and he was not sedated. This case report points towards another area of EMS research that is wide open - IN ketamine for acute pain - what is the right dose and is this safe enough for BLS delivery?
In 2019 Andolfatto et al published a well designed RCT in the EMS
setting comparing IN ketamine to placebo in patients with pain scores
over 5. IN ketamine was not just used in trauma patients like most pain
studies, instead they included a variety of different causes of pain
making it applicable to a broader EMS population. Using a relatively low
dose of IN ketamine (0.75 mg/kg) they found clinically significant
decreases in pain scores in 76% of cases (compared to 41% in placebo
arm). The medics who administered this drug were not the advanced
practice paramedics in the system.
Editorial commentary: I think this is a really important paper
in EMS for three major reasons. First it was on all comers (chest pain
excluded) not just trauma cases so it demonstrates the broad utility of
IN pain medications in EMS.
Second it used a non-sedating drug that does not cause respiratory
depression - eliminating the opiate respiratory depression concern,
potentially improving safety, at the least reducing opiate usage. I can
envision this becoming a therapy that non-paramedic providers will
safely and effectively administer in the not too distant future (as was
the case in this study where it was delivered by non-paramedic EMTs).
Finally, part of the problem with IN medications for pain control in
adults has been that IN fentanyl (great in kids) is too dilute to be
reliably effective in larger adults – especially those who have any
experience with drugs. Sufentanil works great in these cases but is so
potent that it probably will not ever be an EMS drug due to risk of
death if it is stolen. So finally we have an effective drug for IN pain
control in adults with EMS data to support it (and a lot of ER data to
support it as well).
Tanguay et al noted nasal fentanyl to be an effective, safe and superior
delivery technique compared to subcutaneous fentanyl
for pain management in adults
over 70 years of age in the EMS system.
Intranasal opiates (diamorphine, fentanyl) for sickle cell crisis
The management of sickle cell crisis is dependent on immediate pain control, often requiring injectable opiates to achieve success. Unfortunately, sickle cell patients present to the emergency room so often in crisis that their veins are often damaged and it is very difficult to obtain rapid IV access - leading to delays in treatment and excessive nursing resources to gain IV access. An obvious solution given the information presented at this web site is intranasal opiates titrated to effect. Telfer et al report their findings from an observational trial comparing intranasal diamorphine plus IV morphine in 9 patients to intranasal diamorphine plus oral morphine in 13 patients.[49] By 15 minutes, adequate pain control was achieved in 89% of the IN plus IV group versus 70% of the IN plus oral group. At 30 minutes it was 100% vs. 89% and at 120 minutes it was 89% versus 100%. Based on this initial trial, this emergency room has instituted immediate intranasal opiate delivery to all patients presenting in sickle cell crisis, followed by oral opiate medications for longer efficacy. He continues to advocate this humane approach.[107] They report high patient and caregiver satisfaction using this protocol. While diamorphine is not available in many countries, fentanyl and sufentanil are often readily available and there is little reason to suspect it would not be just as effective as diamorphine. Instituting a protocol similar to Telfer's, with the added caveat of allowing titration of repeated IN opiates every 5-20 minutes as needed would greatly reduce suffering, expedite patient care and reduced nursing resource utilization.
Following this publication, a hospital in Ireland was the next to take up the research mantle and they began looking at intranasal fentanyl for treating sickle cell vaso-occlusive crisis.[122] (I found this very curious as I discussed this type of research in the early 2000's with hospitals in the USA where over 50% of their patients were of African descent and they failed to become interested, yet we find a primarily Caucasian country doing the next bit of research in a population with relatively little disease prevalence). They published their proposed protocol in 2012 and presented their data a few years later. The table below tells the story - IN fentanyl was equivalent to IV morphine for adequacy of pain control with rapid onset of effectiveness.
Click here for the Barrett full slide presentation
In the next few years some USA hospitals jumped on board - Oakland California, Boston MA, Atlanta GA, Pittsburgh, PA. Data began to emerge from their research in 2014 and 2015:
In October 2015 there was a report from Boston published in the Journal Pediatrics of successful use of IN fentanyl for treating children with acute sickle cell crisis.[119] As with almost every other article that has measured time to pain medication delivery, these authors found IN fentanyl was given in 23 minutes whereas IV opiates took 56 minutes. Time to second dose and to admission or discharge decision was also reduced in the IN group. Finally the number of admissions dropped from 68% to 52%.
They are now looking at this type of a protocol in adults – I hope given
data seen in similar studies and in other authors experiences with IN
fentanyl in adults that these authors consider using IN sufentanil as it
will work much better in the adult population.
Click here for link OR here for MS word document OR here for abstract link
Here is an in-depth slide set from Boston medical center discussing the path they used to develop a more rapid method for instituting pain control in acute vaso-occlusive crisis. PDF click here
Here is a condensed version by the same group specifically focusing just
on IN fentanyl as the initial approach to reducing those time delays:
PDF click here
Another abstract on this same topic was presented by Fein et al at the
American academy of Pediatrics in October 2015 and then published
in 2017.[120] They also
found more rapid delivery of pain medications and pain control
in these children following
introduction of IN fentanyl (2 ug/kg single dose). Their study had
significant design flaws (no titration, placebo arm got IV opiates, low
doses of drug - but still showed promise for IN fetanyl. Both these articles
support the idea of using intranasal fentanyl as a bridge therapy
allowing more rapid reduction in pain for patients suffering vaso-occlusive
crisis while more standard IV interventions are being instituted. In
other words – give the patient a dose of IN fentanyl as soon as you determine they need pain
medication, then move on to establishing IV access and beginning more
definitive interventions.
Researchers in Atlanta are working on similar protocols, presenting their data at the American society of Hematology meeting in Dec 2014.[121] In a study of close to 200 patients, they too found much faster time to delivery of pain meds in patients receiving IN fentanyl vs. those who did not (29 minutes versus 77 minutes) but with the limited data presented it appears they did not show a reduction in the patients pain scores. When using an opiate for pain this usually implies an erroneous dose. Personally, I think they did not start with a high enough dose and did not repeat it until pain control was significantly improved. Furthermore, as patients size and age increases, I move to a more potent analgesic – sufentanil. Never the less this is a big study and shows that this concept is feasible and we just need to work out the details and dosing a bit better to improve our ability to quickly relieve the suffering that is occurring.
Akinsola et al describe their experience with instituting a nurse initiated IN fentanyl pathway for sickle cell vaso-occlusive pain episodes. They found it resulted in reductions to first dose of pain medication compared to those who did not get IN fentanyl (29 vs. 77 minutes) and high patient/parent and nurse satisfaction with no negative side effects in approximately 200 patients they treated. Following this QI project they instituted the protocol across three large pediatric emergency departments.[138] (Open access - click her for paper)
Kelly et al retrospectively
reviewed 487 ED visits for sickle cell vaso-occlusive crisis, comparing
clinical results of patients who were given IN fentanyl (376 children)
with those given traditional IV medications (111 patients). Those given
IN fentanyl had a shorter time to pain medication administration (29 vs.
78 minutes), higher percentage getting pain medication within 30 minutes
(67% vs. 5%), reduced time to disposition decision (237 vs. 276 minutes)
and reduced LOS (316 vs. 363 min). The retrospective nature of the study
limits definitive conclusions but mirrors those results found for
pediatric extremity injuries in randomized trials.
Myrich et al noted that following the introduction of intranasal
fentanyl to their outpatient sickle cell clinic they were able to
deliver the first dose of opiates more rapidly, they used less morphine
and they admitted fewer patients to the hospital.
In summary, it appears that IN opiates are an effective rapidly initiated initial treatment for pain associated with acute sickle cell induced vaso-occlusive crisis. The exact doses, titration time table and appropriate drug (for children, teenagers and adults) are still being determined, but at this time at a minimum intranasal fentanyl at 1.5 to 2.0 mcg/kg, titrated at least once within 5-10 minutes is safe and equivalent to IV morphine, but much more rapidly delivered.
Intranasal medications for Burn dressing changes:
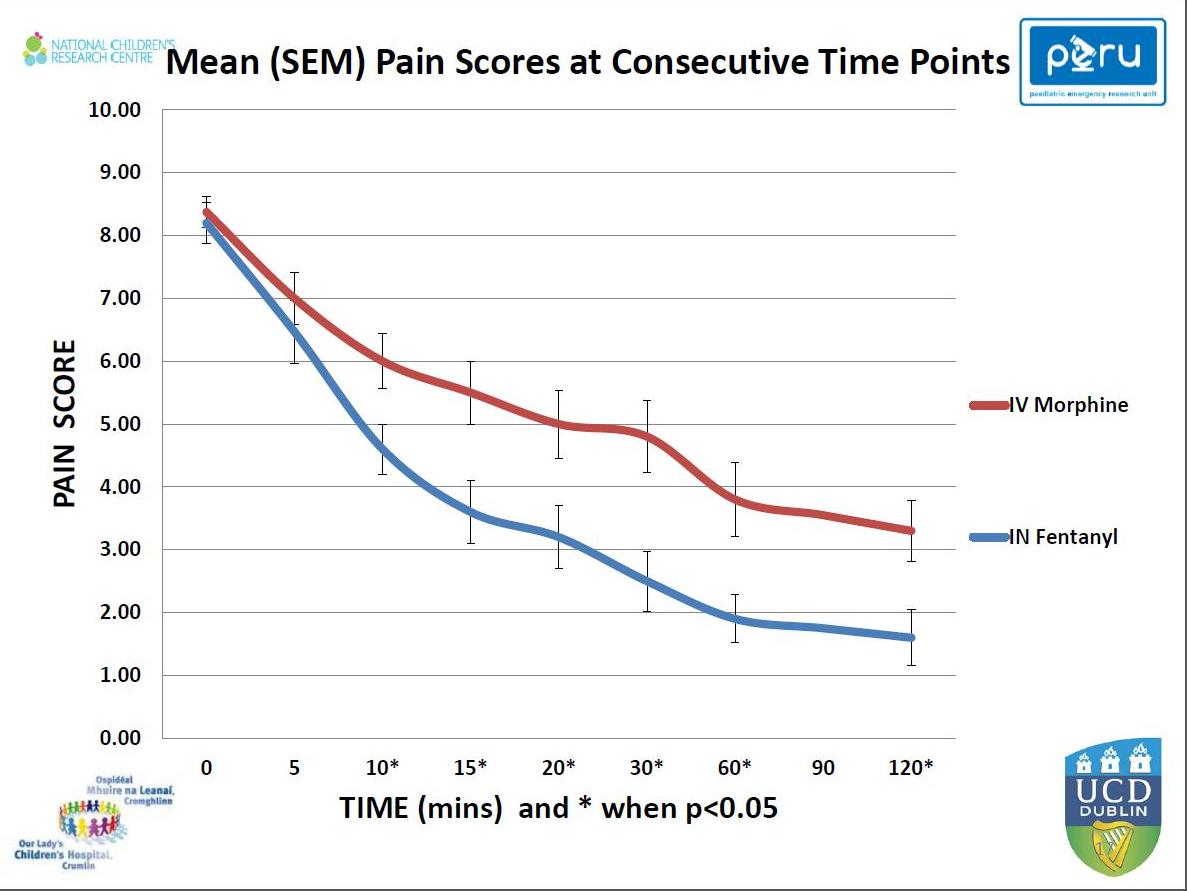
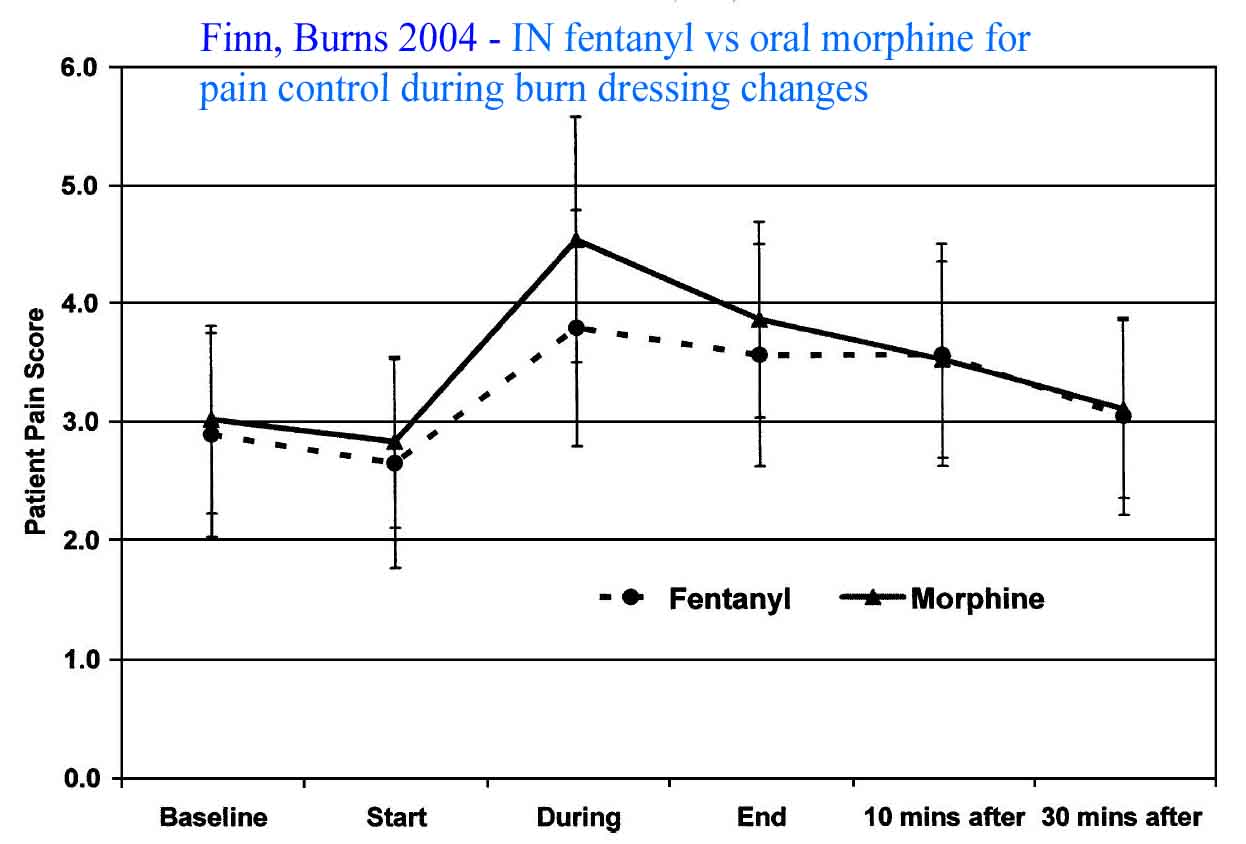
Finn and colleagues compared IN fentanyl to premedication with oral morphine prior to burn wound dressing changes.[45] They found small incremental titrated doses of IN fentanyl equivalent in pain control to pre-medication with oral morphine and felt it was an acceptable alternative that was more easily titratable. Borland et al found similar results with nearly identical conclusions in a population of children requiring burn dressing changes.[46]
Kulbe found low dose intranasal ketamine to be very effective for treating pain associated with burn dressing changes.[59] Since the dose necessary for pain control is about 10 to 15 times less than that needed for sedation, ketamine is often an appropriate drug in situations where opiates are not effective or their side effects cannot be tolerated.
Intranasal Ketorolac
Intranasal ketorolac is also quite effective for treating painful conditions (and recently gained FDA approval). Initial studies showed peak levels around 30-45 minutes with half life of 5-6 hours and bioavailability over 70%.(68, 69) In postoperative patients, 30 mg of intranasal ketorolac results in marked decreases in pain scores and over 30% reduction in opiate use.(70-72) Similar findings occur in patients using intranasal ketorolac for post-dental extraction pain.(73)
Intranasal Ketamine for acute pain
Ketamine is labeled as a general anesthetic drug and in anesthetic doses causes a dissociated catatonic state where patients stare into space – seemingly awake, breathing – but they do not react to painful stimuli. In these doses it can be used for very painful procedures such as joint and bone reduction and other orthopedic and plastic surgical interventions. However, ketamine is also an analgesic drug and demonstrates analgesic properties at doses 10-15 times less that that required for anesthesia. Because of this analgesic effect at low doses, patients often remain completely awake and alert while obtaining substantial relief of their pain. Several studies now confirm the analgesic effect of ketamine in low doses when used to treat painful conditions as well as during dressing changes.[57, 59, 60, 87-91]
The following text reviews currently available literature on this topic:
Kulbe 1996:
This short article is really a case report confirming that intranasal
ketamine spray can be effective for acute pain control during burn
dressing changes. [59] It is
interesting but offers little in terms of dosing
- only suggesting this is an area that deserves further research.
Kaube 2000:
Kaube tested 25 mg of intranasal ketamine in 11 patients with severe
disabling neurologic deficits due to migraine aura finding that about
half the time the nasal ketamine was effective in reducing both severity
and duration of the symptoms.[87]
Editorial
comment - Other migraine
researchers have found intranasal lidocaine occasionally effective for
aborting migraines – perhaps a
combination of lidocaine with ketamine (I suggest 50 mg ketamine) might
be an effective first step therapy to abort a migraine patient visiting
the emergency room. If this fails, progression to more time consuming
and complex therapies can then proceed.
Carr 2004:
Carr found doses of up to 50 mg of IN ketamine were effective in many
patients with difficult to control breakthrough pain (mean pain score
reductions of about 23 mm on a 100 mm VAS).[60]
There was some mild dizziness and feeling of unreality. They conclude
that IN ketamine is safe and effective for augmenting pain control in
this population but that further investigation is necessary.
Christensen 2007: Christensen investigated intranasal ketamine for treating post-operative pain following wisdom tooth removal. [88] Adult patients were randomized to placebo and doses of 10, 30 or 50 mg of intranasal ketamine. They found that “meaningful pain relief was achieved by 14 minutes in 70% of patients receiving the 50 mg dose of IN ketamine. Peak analgesic effect (44 mm drop on VAS) was at 30 minutes.
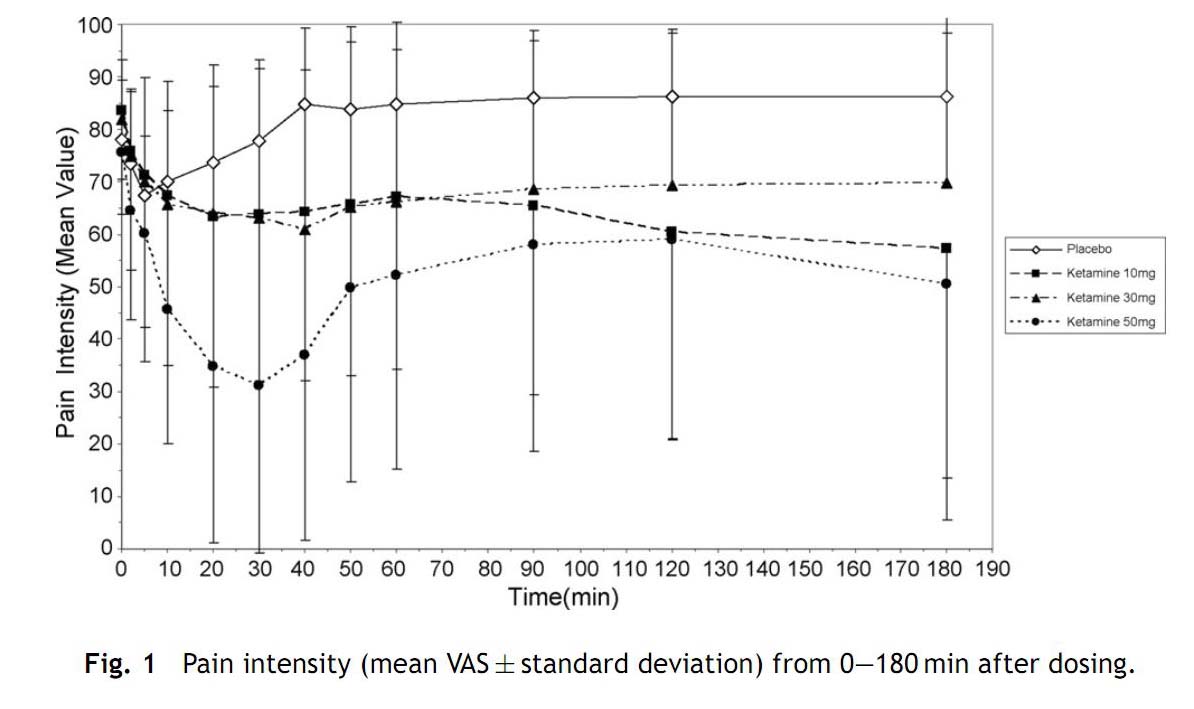
Figure demonstrating rapid reduction in pain scores using 50 mg of IN ketamine in adults.
There was some feeling of unreality and or visual
changes side effects noted in about 50% of patients who received the 50
mg dose which tended to resolve within an hour. The authors report prior
data showing Ketamine bioavailability of their formulation (0.1 ml = 10
mg) of about 33%.
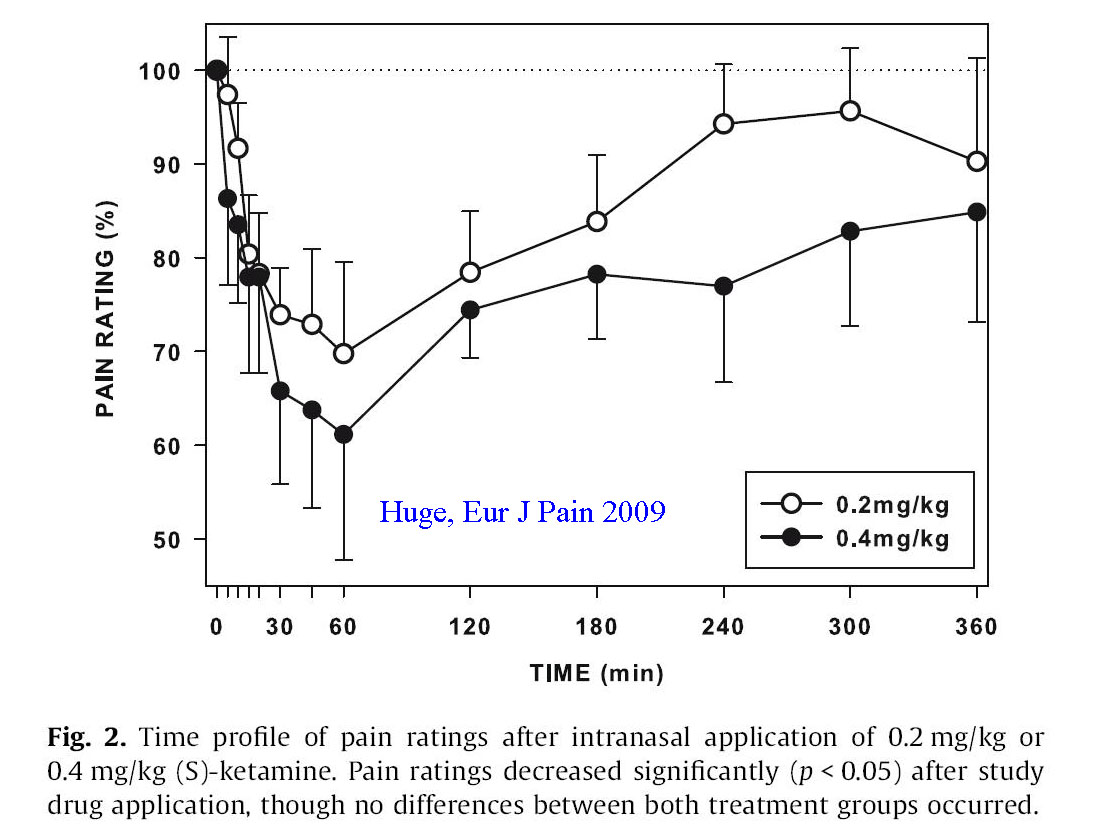
Huge 2009:
This was a small study investigating the pharmacokinetics of low doses
of intranasal ketamine as well as its impact on pain control and the
resulting side effects.[57] The
authors studies 16 patients with chronic neuropathic pain, randomizing
them to either 0.2 mg/kg or 0.4 mg/kg of a dilute form of ketamine (25
mg/ml). Measured serum levels of ketamine peaked at 15 minutes
indicating rapid absorption. Although the doses were low, a measurable
impact on pain control occurred within 15 minutes and peaked at 60
minutes, lasting several hours. Mild to moderate dose dependent side
effects were common, consisting of vertigo, concentration difficulty,
blurred vision and some sedation, though measured cognitive ability was
never impacted.
Reid 2011:
Reid et al report the successful
use in intranasal ketamine in a prehospital setting to treat severe pain
in a child with a 3% scald burn.[89]
They used low dose ketamine (between 0.25 and 0.5 mg/kg) and noted onset
within 3 minutes. There was minimal side effects (no dysphoria, some
swimmy feeling). They conclude that more investigation is necessary for
this promising intervention.
Goudas 2002
abstract: In this RCT patients received either IN ketamine (10 mg
per spray up to 50 mg maximum per event) or placebo for breakthrough
pain.[90] The group using ketamine had markedly better control of pain
within 5 minutes and never needed rescue analgesia. There were no
serious side effects though 20% of the ketamine cases reported feelings
of unreality.
Kronenburg
2002: This study is a
review of ketamine in a variety of administrative formulations
(including nasal) demonstrating that subanesthetic doses result in good
pain control without significant side effects.
[91] It is a bit dated now but
contains a fair amount of interesting data.
Abdel-Ghaffar 2012: This RCT comparing IN ketamine (1.5 mg/kg) vs. IN fentanyl (1.5 mcg/kg) for controlling postoperative pain following FESS sinus surgery showed equivalent pain control (much better than placebo) with a slight increase in dissociative side effects in the Ketamine group.[93]
Afridi 2013: RCT on IN ketamine (25 mg) vs. IN midazolam (2 mg) for migraines showed reduced severity of migraine in the ketamine group.[92]
Yeaman 2013: Yeaman et al conducted a preliminary trail
with sub-dissociative doses of intranasal ketamine to determine a safe
and effective dose to treat pain related to acute limb injury in
children.[94] This prospective dosing trial entered 30 patients weights
10-50 kg who had pain scores of 6 or higher. In an open label fashion
they all received an initial dose of about 0.7 mg/kg of ketamine (100
mg/kg diluted to exactly ½ ml – half up each nostril with an atomization
device). At 15 minutes their pain was reassessed and at the clinicians
discretion another dose of 0.5 mg/kg was administered. Pain scores were
obtained at 0, 30 and 60 minutes. Degree of sedation and side effects
were also recorded. 28 patients completed the trail, 10 received a
second dose of ketamine at 15 minutes. The mean total dose of ketamine
given to all patients was 1 mg/kg. Pain scores for the group at entry,
30 and 60 minutes were 74.5, 30 and 25 mm on a 100 mm scale. Minimal
sedation occurred in 12 patients at 30 minutes but was gone by 60
minutes. Very mild side effects that did not need treatment and were
transient were noted- dizziness in 36%, dysphoria in 14%. No patients
suffered dissociation or hallucinations. 83% of patients were satisfied
with the degree of pain control. The authors conclude that intranasal
ketamine in sub-dissociative doses is effective for moderate to severe
pain associated with orthopedic injury, they recommend future studies
start with a dose of 1 mg/kg since it is safe and effective. They
suggest this therapy be an alternate or a complementary analgesic choice
for IN administration in children with acute pain.
Editorial
comment: Here is the first study that many readers have been awaiting
describing the efficacy of intranasal ketamine for treatment of acute
pain. It is a small, preliminary trial but the results are promising and
it gives us a starting dose – 1 mg/kg of intranasal ketamine. This drug
might be used to complement fentanyl if the initial dose of fentanyl is
effective, or vsa versa – given first line and followed with Fentanyl if
additional pain medication is required. The study also points out a
concept that some clinicians still are not familiar with – the concept
of titration of pain medication via the NASAL route just as we all do
via the intravenous route. Within 30 minutes, using no IV access, these
children had their pain scores down by 44 mm. This is almost identical
to that seen with titrated fentanyl in the Borland study from 2007. Here
is another tool in our armamentarium for treating acute pain –
painlessly.
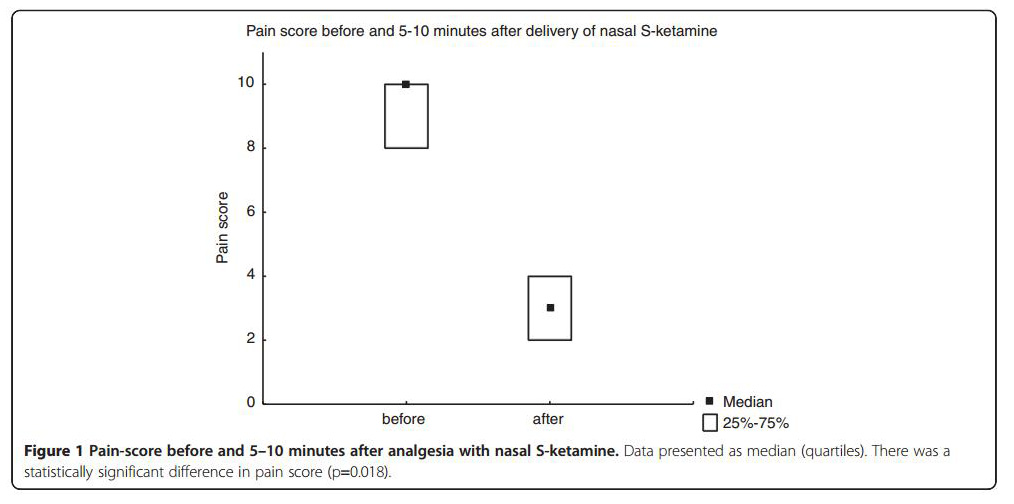
The authors conclude: “To summarize, the opinion of our experienced
prehospital staff was that nasal S-ketamine offered a fast, easy, and
essentially non-invasive way of reducing acute pain secondary to trauma,
without appreciable side effects…. “Further advantages are a relatively
low cost of the treatment, a needleless approach that diminish the risk
of transmission of blood-borne infections, and supposedly a reduced
rescue-time which is particularly valuable in a cold or otherwise
dangerous environment.”
Shrestha 2016: Shrestha et al conducted a cross sectional
observational study of patients who were given IN ketamine (0.7 mg/kg
initially, 0.3 mg/kg at 15 minutes if pain scores still exceeded 50 mm)
for severe pain in the emergency department. They entered 34 patients
and found VAS scores reduced from 80 mm to 40 mm (15 min), 20 mm (30
min) and 20 mm (60 minutes). 80% of patients had clinically significant
pain score reductions by 15 minutes. The conclude that IN ketamine is an
option for pain control in a busy or resource limited ED.
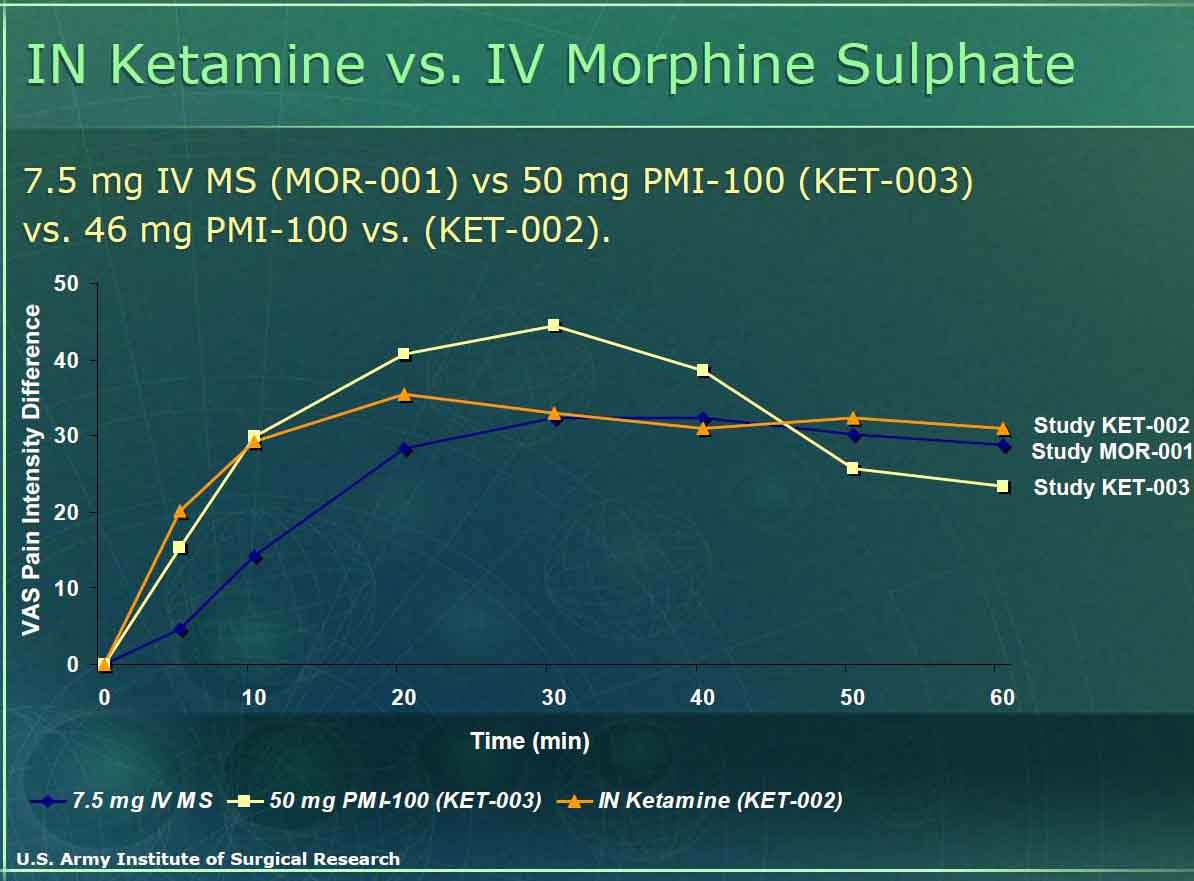
The U.S. military may be the group most interested in intranasal ketamine for treating acute pain. This group is looking for a pain medication that can be self administered and relieve a soldiers acute pain related to war injury, yet let him/her still function at a high level and either be able to extricate himself or finish the mission (often saving his/her life and others by being a functional asset rather than a detriment). To date they have funded and conducted numerous studies to find the right dose of IN intranasal ketamine while determining the incidence of side effects. Looking at the material posted on the internet, they have studied at least 117 subjects with doses ranging from 10 to 50 mg of ketamine finding no serious effects and adequate pain control. The graph above notes their results in terms of dosing equivalency – finding 50 mg of nasal ketamine as effective or more effective than 7.5 mg of IV morphine without the loss of function seen with morphine. Look for more literature on this topic in the near future. (click here for military report from the internet in 2005)
Click here for a 2009 review of combat pain control
Click here for a slide set 2010 review of ketamine
Summary:
While dissociative sedation with Ketamine requires fairly high doses of
drug (10 mg/kg to be reliable - see
sedation section) it appears that about
1 mg/kg of nasal ketamine (or
simply 50 mg in an adult) is quite effective for pain control without
substantial sedation. Many patients do feel a bit dysphoric, but their
cognitive functions remain intact.
Using the generic formulation of ketamine at 100mg/ml would make
nasal volumes ideal for atomization at this dose. It will be interesting
to see if further research in the acute setting such as remote clinics,
prehospital setting (where
generic fentanyl is a bit dilute for adult pain control), battle field
setting and emergency room validate this concept. Especially interesting
to those of us in the hospital will be for use in conditions such as
migraines and chronic pain situations where treatment with an opiate has
significant clinical downsides.
Break-Through pain:
See separate extensive Hospice section as well (click here)
This section of the website is no longer updated as these are now mature, FDA approved products (pricy but highly concentrated and effective though a bit more risky due to that high concentration - especially if kids accidently inhale while copying the adult who needs the drug. Hundreds of articles per year are available on PubMed)
Break-through pain is a complex problem affecting many patients and is widespread among patients suffering from cancer. Ideally this condition could be treated with a medication that is easy to use by a lay person, has rapid onset and is short in duration. In addition many of these patients have problems with nausea, swallowing and dry oral mucosa making oral and sublingual opiates suboptimal. Not surprisingly, intranasal opiates offer an attractive solution to this complex problem. Their onset is within a few minutes – comparable to intravenous medications, yet they can be easily delivered by a lay person even if the person has dry oral mucosa or is nauseated. Too date, the published literature on the subject is limited but many large trials are ongoing. It is likely that in the near future numerous intranasal opiate formulations will be available commercially. However, generic medications already exist, have been found to be effective in small patient cohorts and can be inexpensively implemented now in the appropriate patient setting.[7, 17, 47]
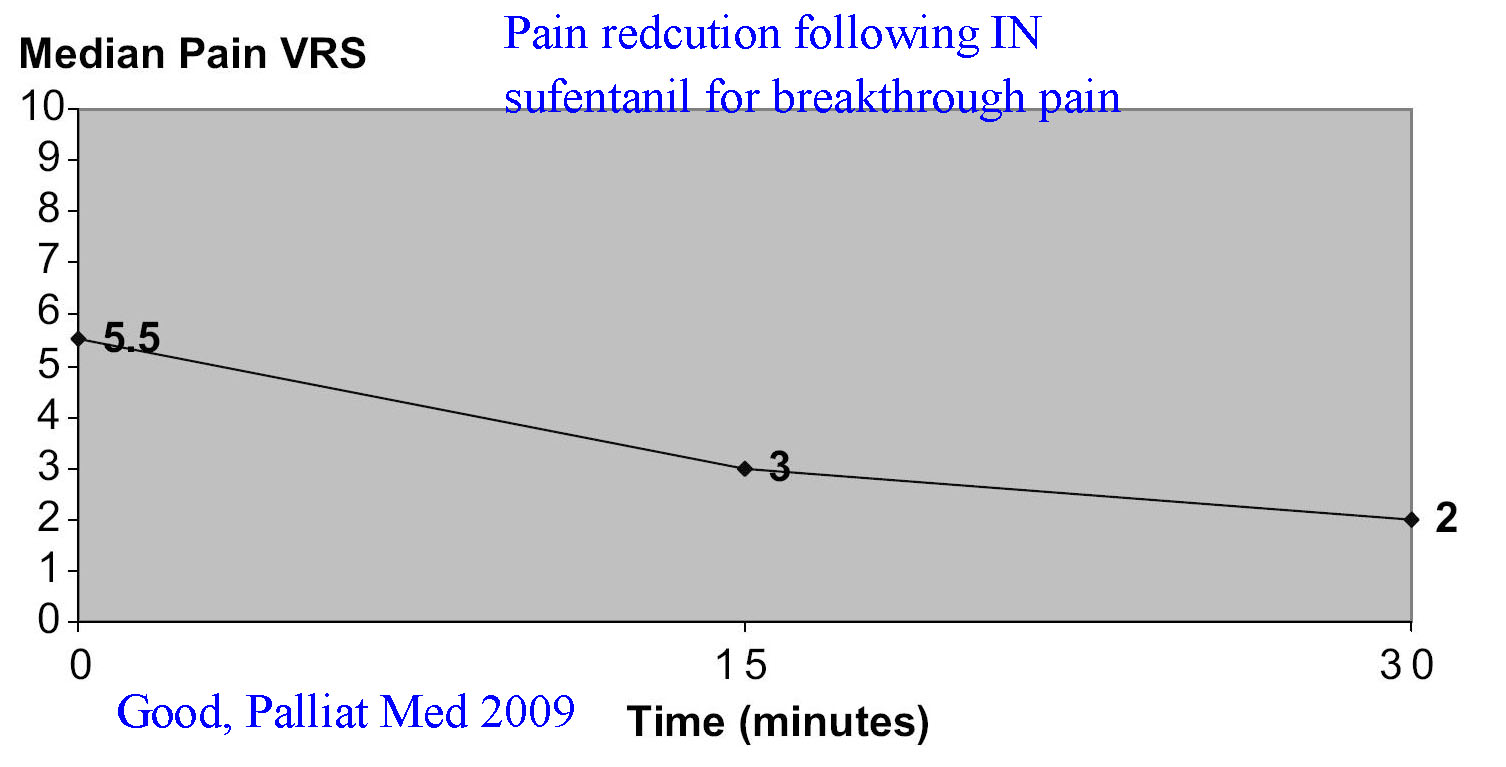
(click here for a link to a palliative pain and dyspnea protocol)In 2009 two important studies were published investigating the use of intranasal opiates for the treatment of breakthrough cancer pain and a third was published investigating intranasal ketamine for breakthrough neuropathic pain.[55,56,57]
Good et al studied intranasal sufentanil effectiveness for treating breakthrough pain in cancer patients.[55] The investigators first step was to determine the effective and safe dose of nasal sufentanil by incrementally increasing the dose administered until an effective but non-sedation dowse was determined (dose titration phase). They found the mean effective dose to be about 20 mcg with a range of 9 to 108 micrograms per dose. They then sent the patients home with the delivery device and allowed them to administer intranasal sufentanil as needed for breakthrough pain. The bottom line – 77% found it as effective as prior medications and 94% preferred it as their first line treatment for breakthrough pain. The authors conclude that intranasal sufentanil “provides acceptable and often preferred breakthrough analgesia for many patients and most importantly, it can provide rapid pain relief. This study also showed that IN sufentanil can be used safely, with a very low incidence of adverse effects, in an inpatient palliative care population. We suggest that IN sufentanil be added to the armamentarium of medication used to treat breakthrough pain with the proviso that it requires an initial dose titration phase.”
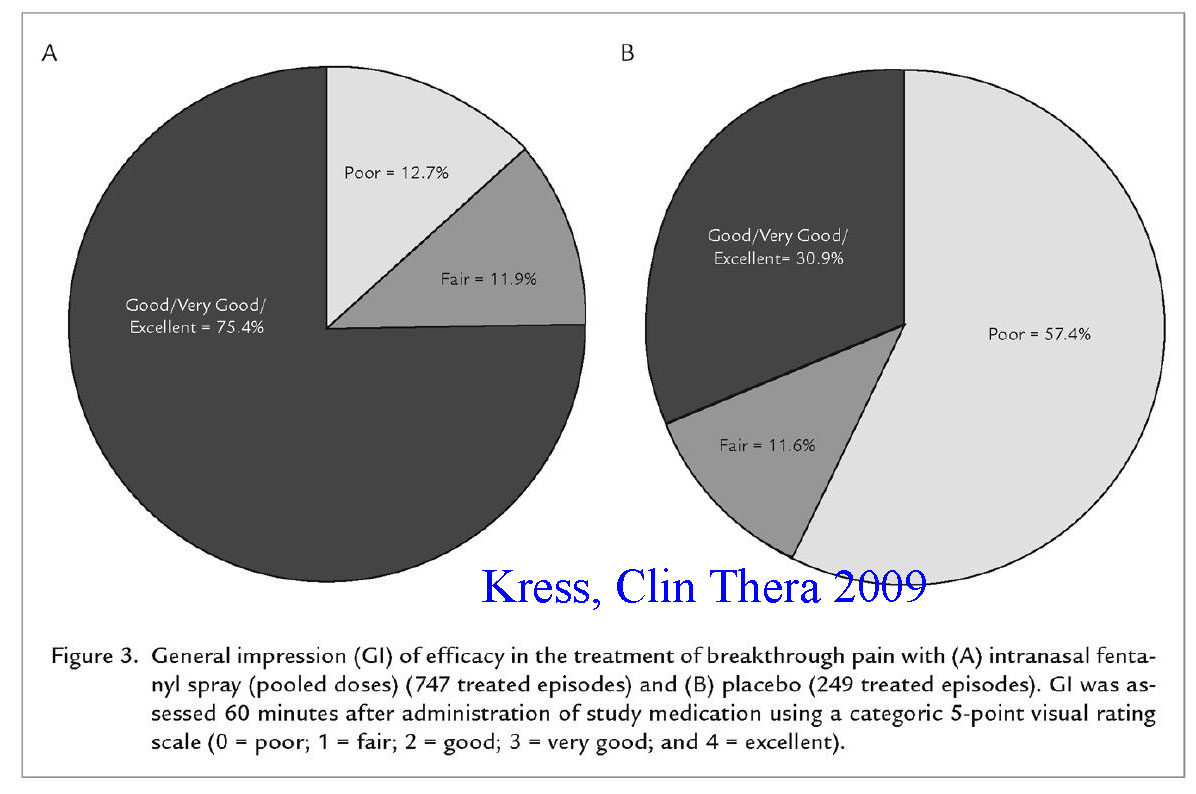
Kress et al
conducted a multinational randomized, double blind, placebo controlled
trial investigating intranasal fentanyl (compounded into increasingly
potent doses) for the management of cancer breakthrough pain.[56] They
also conducted a dose
titration phase (to find the proper individual dose) prior to study
entry and found intranasal opiates to be effective (see diagram) in
cancer breakthrough pain within a few minutes. Nausea and vertigo were
the most common side effects noted. No respiratory side effects were
noted.
Finally, Huge et al investigated intranasal ketamine in the treatment of chronic neuropathic pain.[57] The authors used relatively low doses of this medication since they had no desire for sedation, instead simply wanted NMDA receptor antagonism to suppress neuropathic pain. Used doses of 0.2 to 0.4 mg/kg they noted substantial reductions in pain (dose related – see diagram). They conclude that low-dose intranasal ketamine is a feasible method to produce rapid onset analgesia for neuropathic breakthrough pain conditions.
Intranasal flumazenil and intranasal naloxone as a reversal agents in sedated patients without an IV line
A concern that often comes up regarding administration of sedatives and opiates to patients who are given these powerful drugs via the intranasal route is how they can be reversed should too much sedation develop (since they presumably do not have an intravenous line). The first point that needs to be considered is whether significant respiratory depression requiring intervention beyond oxygen therapy will even occur from intranasal drug delivery. To date it has not been reported for midazolam and it does not seem common even with very high doses of the extremely powerful drug sufentanil (it does occur with sufentanil at times). This is probably because the medications absorb via the nasal mucosa are spread out over 10-15 minutes and never achieve peak levels seen with intravenous boluses (see detailed discussion on therapeutic threshold and side effect threshold concept above). Never the less, antidotes to opiates - i.e. naloxone - work very well intranasally as well as via subcutaneous and intramuscular routes (see separate section on this topic - click here). In terms of intranasal flumazenil - the benzodiazepine antagonist - there is limited data but that which exists also suggests that it is effective when administered via the nasal route. Two animal studies found transmucosal flumazenil delivered via the sublingual route resulted in rapidly measurable serum drug levels that achieved the therapeutic threshold and approached 100% bioavailability.[51,52] One of these studies actually demonstrated reversal of benzodiazepine induced sedation about 4 minutes after drug delivery.[51] Two human studies exist in children using flumazenil intranasally Scheepers found maximal concentrations in the serum were achieved very quickly (2 minutes), again at therapeutic blood levels and concluded that this may offer an alternate delivery route for benzodiazepine antagonist reversal agents.[53] Heard et al presents a case where and child undergoing a dental procedure was oversedated using intranasal midazolam combined with intranasal sufentanil. [54] The authors responded to this problem by administering 0.4 on intranasal naloxone and 200 mcg of intranasal flumazenil. Three minutes following antidote administration the pati9ent was fully awake and did not become re-sedated during the next 2.5 hours of observation.
Personal insights from experienced clinicians
Pat Crocker, DO, Chief of Emergency Medicine, Dell Children's Medical Center, Austin TX.... We have had great success with IN fentanyl for immediate pain control in children and it is much quicker than waiting for an iv to be established. Giving the fentanyl IN immediately and applying some topical anesthetic cream makes subsequent iv insertion less traumatic for the child as well.
The combination of IN fentanyl and Versed prior to minor procedures and administration of local anesthetic has been quite useful as well. No child has fallen asleep at the suggested doses but generally is quite a bit more tractable for the procedure reducing our need for full sedations some. We have also combined the above with nitrous oxide for children 5 yo and older and get nice results.
Tom Macfarlane, MD, Staff Emergency Physician, Jordan Valley Hospital, Salt Lake City UT …When a patient presents with an acutely painful condition increasingly I am reaching for an intranasal opiate to treat their pain. In both children and adults with clinical long bone fractures I am able to substantially control their pain within a few minutes of arrival with IN opiates. Abscesses, burns and joint dislocations are some of the other conditions that respond very well to IN analgesia. The IN route of administration has several advantages that I feel are very important. It is very fast. Onset is typically apparent in less than a minute after administration. It is painless and this is especially appreciated by children and their families. The IN route keeps a patient NPO in case they need sedation or need to go to the operating room. And lastly, it is very effective and titratable. Overall this is an excellent means to control acute pain in the emergency department.
Treatment protocol
Indications:
- Adult and pediatric minor painful injuries or procedures:
- Orthopedic trauma not requiring an IV (or prior to starting an IV)
- Anytime pain control is needed but oral medication is too slow
- Burn dressing changes
- Re-packing wounds such as abscesses
- Any time you consider an IM shot for pain control (IN works as well or better with faster onset and no pain on delivery)
Dosing and method:
- Fentanyl, sufentanil or diamorphine are most appropriate for IN
delivery to treat pain
- Reasonable IN starting dose for painful procedures:
- Fentanyl: 2 ug/kg (comes in 50 ug/ml, you can ask your
- Reasonable IN starting dose for painful procedures:
Strongly consider administering an oral pain medication at the same time as the nasal medication. This way as the effect of the nasal drug wanes, the effect of the oral medication begins to have an effect.
Naloxone is effective intranasally if you need a reversal agent
Be aware that there is often a "dead space" within the delivery device you use - this leads to some of the drug remaining within the device and not being delivered to the patient. Be certain to draw up that extra volume into the syringe to account for the dead space that will remain.
Dosing tables (to assist with volume calculations)
Generic Fentanyl dosing table
Fentanyl (generic) is most appropriate for children since it becomes too dilute as the child's weight (and therefore the volume delivered) increases.
Dosing Plan: Fentanyl concentration - 0.1ml = 5 mcg (50 mcg/ml)
Comment: A very simple way to calculate the dose is as follows:
Dose in ml = kg weight x 4/100 plus 0.1 ml dead space
or simply Dose in ml = kg weight x .04 plus the 0.1 ml dead space
|
You should draw up the additional appropriate dead space of the delivery device you choose. In this table the 0.1 ml represents a typical dead space in a 1 ml syringe connected to a syringe driven atomizer.
**If the volume exceeds 1 ml you might want to consider using sufentanil instead.
# Volumes in this range should be divided in half and administered 10 minutes apart to reduce runoff. It would likely be more appropriate to use sufentanil if that is available.Generic Sufentanil dosing table
Sufentanil is more appropriate for adult patients because it is so concentrated that it is difficult to measure for small children. It comes in 50 mcg/1 ml vials. Occasionally you will need two vials for adequate dosing.
Dosing Plan: Sufentanil concentration - 0.1ml = 5 mcg (50 mcg/ml)
|
*The volumes are rounded up to the nearest 0.05 ml and you should draw up the additional appropriate dead space of the delivery device you choose. In this table the 0.1 ml represents a typical dead space in a 1 ml syringe connected to a syringe driven atomizer.
It is best to use a 1 ml syringe to draw up this drug so you get accurate measurements.
**If the volume exceeds 1 ml, you will need to simply administer a lower mcg/kg dose (just give the entire 50 mcg vial) and re-assess in 10 -12 minutes at which point you can administer additional medication from a second vial. You may also simply obtain a second vial and a second syringe (or draw it up in a 3 ml syringe) at the outset and administer the entire volume at once– you can switch a nasal atomizer from one syringe to the second syringe.
Small Children should probably have fentanyl used rather than sufentanil to simplify the dosing volumes.
Dosing tables in Non-English language
Deutsch / German language
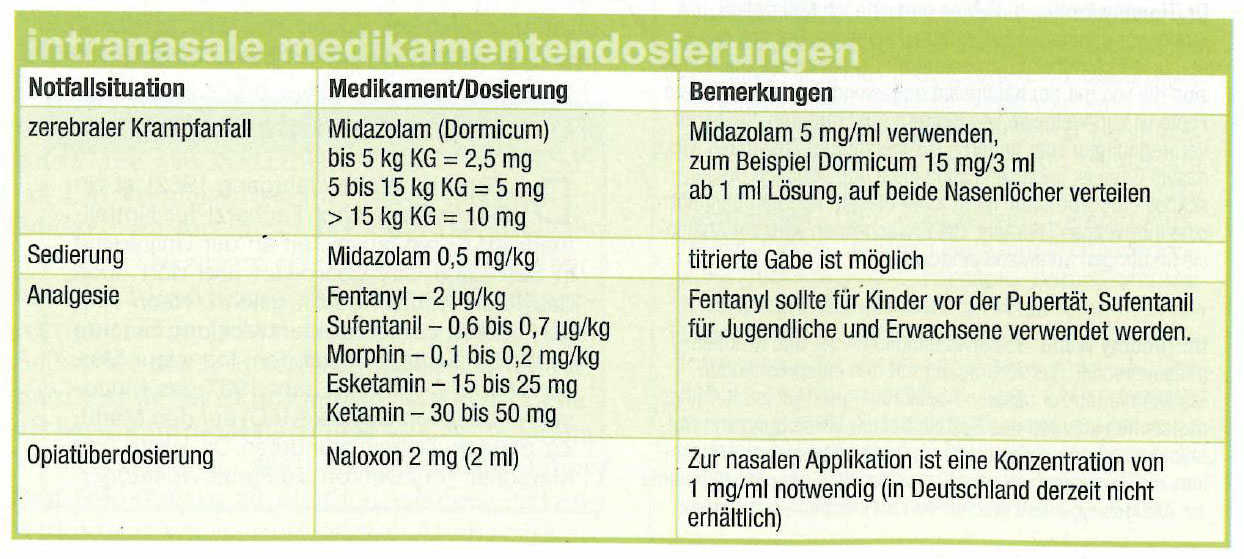{kind=link}
Deutsch 2 (Editors note: the doses are too low for fentanyl and morphine - double the dose these chart recommends for better effect that is still safe - see above literature)
Italia / Italian language
Diamorphine dosing table
Diamorphine is supplied as a powder and needs to be re-concentrated in a diluent prior to administration. The following link will connect you to a web site that provides directions for reconstitution. Be aware that this link assumes you will be administering the drug to one nostril and that you will use a dropper to administer the medication. If you use an atomizer you must add the additional dead space of the device or you risk under dosing the patient
Leeds Hospital IN diamorphine protocol (click here)
NHS intranasal diamorphine protocol for UK (click here)
Teaching materials:
Intranasal sufentanil delivery photo guide (click here) - Word document
Intranasal sufentanil delivery photo guide (click here) - PDF document
Intranasal fentanyl delivery photo guide (click here) - Word document
Intranasal fentanyl delivery photo guide (click here) - PDF document
What's new in pediatric emergency rooms - IN fentanyl for pain (click here) - Dr. Malcolm Higgins - PDF document of Power Point Slides
Intranasal fentanyl in pediatric emergency rooms (click here) - Sally Britnell, RN presentation - PDF of Power Point slides
EMS and ER protocol for Intranasal fentanyl
Peer Reviewed articles:
Intranasal Morphine for pain
Fitzgibbon, Nasal Morphine for breakthrough pain, Pain 2003 (click here) - PDF 0.15 MB
Intranasal Fentanyl for pain
Intranasal Sufentanil for pain
Heshmati, Intranasal sufentanil for postoperative pain control in lower abdominal pediatric surgery, IJPT 2006 (click here) - PDF 0.14 MB
Matheiu, Intranasal sufentanil is effective for postoperative analgesia in adults, Can J Anaesthesia 2006 (click here) - PDF 0.32 MB
Intranasal Diamorphine for pain
Intranasal ketamine for pain
Nose brain pathway delivery of pain medications:
Westin, Olfactory transfer of analgesic drugs after nasal administration, 2007
Bibliography (click here for abstracts)
-
CDC, National Hospital Ambulatory Medical Care Survey: 1998 Emergency Department Summary. CDC website, 2000: p. www.cdc.gov/nchs/data/ad/ad313.pdf.
-
Stanley, T.H., Anesthesia for the 21st Century. BUMC Proceedings, 2000. 13: p. 7-10.
-
Striebel, H.W., J. Pommerening, and A. Rieger, Intranasal fentanyl titration for postoperative pain management in an unselected population. Anaesthesia, 1993. 48(9): p. 753-7.
-
Striebel, H.W., et al., Self-administered intranasal meperidine for postoperative pain management. Can J Anaesth, 1995. 42(4): p. 287-91.
-
Wilson, J.A., J.M. Kendall, and P. Cornelius, Intranasal diamorphine for paediatric analgesia: assessment of safety and efficacy. J Accid Emerg Med, 1997. 14(2): p. 70-2.
-
Kendall, J.M., B.C. Reeves, and V.S. Latter, Multicentre randomised controlled trial of nasal diamorphine for analgesia in children and teenagers with clinical fractures. Bmj, 2001. 322(7281): p. 261-5.
-
Jackson, K., M. Ashby, and J. Keech, Pilot dose finding study of intranasal sufentanil for breakthrough and incident cancer-associated pain. J Pain Symptom Manage, 2002. 23(6): p. 450-2.
-
Striebel, H.W., et al., Patient-controlled intranasal analgesia (PCINA) for the management of postoperative pain: a pilot study. J Clin Anesth, 1996. 8(1): p. 4-8.
-
Striebel, H.W., et al., Patient-controlled intranasal analgesia: a method for noninvasive postoperative pain management. Anesth Analg, 1996. 83(3): p. 548-51.
-
Toussaint, S., et al., Patient-controlled intranasal analgesia: effective alternative to intravenous PCA for postoperative pain relief. Can J Anaesth, 2000. 47(4): p. 299-302.
-
Schwagmeier, R., et al., [Patient acceptance of patient-controlled intranasal analgesia (PCINA)]. Anaesthesist, 1996. 45(3): p. 231-4.
-
PharmacologyFocusTeam, Battlefield pain control: Intranasal ketamine. Cognitive Performance Workshop. 19-25 July 2005: p. https://www.momrp.org/CognitivePerformance/Pharmos/PO5.pdf.
-
Borland, M., et al., A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med, 2007. 49(3): p. 335-40.
-
Borland, M.L., I. Jacobs, and G. Geelhoed, Intranasal fentanyl reduces acute pain in children in the emergency department: a safety and efficacy study. Emerg Med (Fremantle), 2002. 14(3): p. 275-80.
-
Moksnes, K., et al., Early pharmacokinetics of nasal fentanyl: is there a significant arterio-venous difference? Eur J Clin Pharmacol, 2008.
-
Rickard, C., et al., A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting. Am J Emerg Med, 2007. 25(8): p. 911-7.
-
Zeppetella, G., An assessment of the safety, eff icacy, and acceptability of intranasal fentanyl citrate in the management of cancer-related breakthrough pain. A pilot study. J Pain Symptom Manage, 2000. 20(4): p. 253-8.
-
Dale, O., R. Hjortkjaer, and E.D. Kharasch, Nasal administration of opioids for pain management in adults. Acta Anaesthesiol Scand, 2002. 46(7): p. 759-70.
-
Takala, A., et al., Pharmacokinetic comparison of intravenous and intranasal administration of oxycodone. Acta Anaesthesiol Scand, 1997. 41(2): p. 309-12.
-
Wolfe, T., Intranasal fentanyl for acute pain: techniques to enhance efficacy. Ann Emerg Med, 2007. 49(5): p. 721-2.
-
Kendall, J.M. and V.S. Latter, Intranasal diamorphine as an alternative to intramuscular morphine: pharmacokinetic and pharmacodynamic aspects. Clin Pharmacokinet, 2003. 42(6): p. 501-13.
-
Abrams, R., et al., Safety and effectiveness of intranasal administration of sedative medications (ketamine, midazolam, or sufentanil) for urgent brief pediatric dental procedures. Anesth Prog, 1993. 40(3): p. 63-6.
-
Bates, B.A., S.A. Schutzman, and G.R. Fleisher, A comparison of intranasal sufentanil and midazolam to intramuscular meperidine, promethazine, and chlorpromazine for conscious sedation in children. Ann Emerg Med, 1994. 24(4): p. 646-51.
-
Bayrak, F., et al., A comparison of oral midazolam, oral tramadol, and intranasal sufentanil premedication in pediatric patients. J Opioid Manag, 2007. 3(2): p. 74-8.
-
Henderson, J.M., et al., Pre-induction of anesthesia in pediatric patients with nasally administered sufentanil. Anesthesiology, 1988. 68(5): p. 671-5.
-
Karl, H.W., et al., Comparison of the safety and efficacy of intranasal midazolam or sufentanil for preinduction of anesthesia in pediatric patients. Anesthesiology, 1992. 76(2): p. 209-15.
-
Vercauteren, M., et al., Intranasal sufentanil for pre-operative sedation. Anaesthesia, 1988. 43(4): p. 270-3.
-
Zedie, N., et al., Comparison of intranasal midazolam and sufentanil premedication in pediatric outpatients. Clin Pharmacol Ther, 1996. 59(3): p. 341-8.
-
Finkel, J.C., et al., The effect of intranasal fentanyl on the emergence characteristics after sevoflurane anesthesia in children undergoing surgery for bilateral myringotomy tube placement. Anesth Analg, 2001. 92(5): p. 1164-8.
-
Galinkin, J.L., et al., Use of intranasal fentanyl in children undergoing myringotomy and tube placement during halothane and sevoflurane anesthesia. Anesthesiology, 2000. 93(6): p. 1378-83.
-
Manjushree, R., et al., Intranasal fentanyl provides adequate postoperative analgesia in pediatric patients. Can J Anaesth, 2002. 49(2): p. 190-3.
-
Roelofse, et al., Intranasal sufentanil/midazolam versus ketamine/midazolam for analgesia/sedation in the pediatric population prior to undergoing multiple dental extractions under general anesthesia: a prospective, double-blind, randomized comparison. Anesth Prog, 2004. 51(4): p. 114-21.
-
Striebel, H.W., D. Koenigs, and J. Kramer, Postoperative pain management by intranasal demand-adapted fentanyl titration. Anesthesiology, 1992. 77(2): p. 281-5.
-
Striebel, W.H., et al., Intranasal meperidine titration for postoperative pain relief. Anesth Analg, 1993. 76(5): p. 1047-51.
-
Christrup, L.L., et al., Pharmacokinetics, efficacy, and tolerability of fentanyl following intranasal versus intravenous administration in adults undergoing third-molar extraction: A randomized, double-blind, double-dummy, two-way, crossover study. Clin Ther, 2008. 30(3): p. 469-81.
-
Mathieu, et al., Intranasal sufentanil is effective for postoperative analgesia in adults. Can J Anaesth, 2006. 53(1): p. 60-6.
-
Paech, M.J., et al., A new formulation of nasal fentanyl spray for postoperative analgesia: a pilot study. Anaesthesia, 2003. 58(8): p. 740-4.
-
Stoker, D.G., et al., Analgesic efficacy and safety of morphine-chitosan nasal solution in patients with moderate to severe pain following orthopedic surgery. Pain Med, 2008. 9(1): p. 3-12.
-
Ward, M., G. Minto, and J.M. Alexander-Williams, A comparison of patient-controlled analgesia administered by the intravenous or intranasal route during the early postoperative period. Anaesthesia, 2002. 57(1): p. 48-52.
-
Hallett, A., et al., Patient-controlled intranasal diamorphine for postoperative pain: an acceptability study. Anaesthesia, 2000. 55(6): p. 532-9.
-
Abboud, T.K., et al., Transnasal butorphanol: a new method for pain relief in post-cesarean section pain. Acta Anaesthesiol Scand, 1991. 35(1): p. 14-8.
-
Cannon, C.R., Transnasal butorphanol: pain relief in the head and neck patient. Otolaryngol Head Neck Surg, 1997. 116(2): p. 197-200.
-
Gillis, J.C., P. Benfield, and K.L. Goa, Transnasal butorphanol. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in acute pain management. Drugs, 1995. 50(1): p. 157-75.
-
Saunders, M., K. Adelgais, and D. Nelson, Use of Intranasal Fentanyl for the Relief of Orthopedic Trauma Pain. Pediatric Emergency Medicine data base, 2007: p. http://www.pemdatabase.org/PAS2007.html.
-
Finn, J., et al., A randomised crossover trial of patient controlled intranasal fentanyl and oral morphine for procedural wound care in adult patients with burns. Burns, 2004. 30(3): p. 262-8.
-
Borland, M.L., et al., Intranasal fentanyl is an equivalent analgesic to oral morphine in paediatric burns patients for dressing changes: a randomised double blind crossover study. Burns, 2005. 31(7): p. 831-7.
-
Harlos, M., Palliative Care Incident Pain and Incident Dyspnea Protocol. Internet public domain protocol, 2002: p. http://palliative.info/incidentpain.htm.
-
Heshmati, F., et al., Intranasal sufentanil for postoperative pain control in lower abdominal pediatric surgery. Iranian Journal of Pharmacology and Therapeutics, 2006. 5(2): p. 131-133.
-
Telfer, P.T., et al., Intranasal diamorphine for acute sickle cell pain. Arch Dis Child, 2009.
-
Borland, M.L., L.J. Clark, and A. Esson, Comparative review of the clinical use of intranasal fentanyl versus morphine in a paediatric emergency department. Emerg Med Australas, 2008. 20(6): p. 515-20.
-
Heniff, M.S., et al., Comparison of routes of flumazenil administration to reverse midazolam-induced respiratory depression in a canine model. Acad Emerg Med, 1997. 4(12): p. 1115-8.
-
Oliver, F.M., et al., Comparative pharmacokinetics of submucosal vs. intravenous flumazenil (Romazicon) in an animal model. Pediatr Dent, 2000. 22(6): p. 489-93.
-
Scheepers, L.D., et al., Plasma concentration of flumazenil following intranasal administration in children. Can J Anaesth, 2000. 47(2): p. 120-4.
-
Heard, C., P. Creighton, and J. Lerman, Intranasal flumazenil and naloxone to reverse over-sedation in a child undergoing dental restorations. Paediatr Anaesth, 2009. 19(8): p. 795-7.
-
-
-
-
Moodie, J.E., et al., The safety and analgesic efficacy of intranasal ketorolac in patients with postoperative pain. Anesth Analg, 2008. 107(6): p. 2025-31.
-
Kulbe, J., The use of ketamine nasal spray for short-term analgesia. Home Healthc Nurse, 1998. 16(6): p. 367-70.
-
Carr, D.B., et al., Safety and efficacy of intranasal ketamine for the treatment of breakthrough pain in patients with chronic pain: a randomized, double-blind, placebo-controlled, crossover study. Pain, 2004. 108(1-2): p. 17-27
-
Voronov, P., et al., Postoperative pain relief in infants undergoing myringotomy and tube placement: comparison of a novel regional anesthetic block to intranasal fentanyl--a pilot analysis. Paediatr Anaesth, 2008. 18(12): p. 1196-201.
-
Cole, J., M. Shepherd, and P. Young, Intranasal fentanyl in 1-3-year-olds: A prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas, 2009. 21(5): p. 395-400.
-
Holdgate, A., A. Cao, and K.M. Lo, The Implementation of Intranasal Fentanyl for Children in a Mixed Adult and Pediatric Emergency Department Reduces Time to Analgesic Administration. Acad Emerg Med, 2010. 17:p1-4.
-
Crellin, D., R.X. Ling, and F.E. Babl, Does the standard intravenous solution of fentanyl (50 microg/mL) administered intranasally have analgesic efficacy? Emerg Med Australas, 2010. 22(1): p. 62-7.
-
McLean, A.R., et al., Intranasal fentanyl for analgesia in injured patients at a ski resort (abstract). Wilderness Medical Journal, 2009. 21(1): p. 68-69.
-
Han, M., H. Wang, and B. Tong, Intranasal instillation of sufentanil reduces myoclonus induced by etomidate. Anhui Medical and Pharm J, 2009.
-
Johnston S, Wilkes GJ, Thompson JA, Ziman M, Brightwell R. Inhaled methoxyflurane and intranasal fentanyl for prehospital management of visceral pain in an Australian ambulance service. Emerg Med J 2010.
-
McAleer SD, Majid O, Venables E, Polack T, Sheikh MS. Pharmacokinetics and safety of ketorolac following single intranasal and intramuscular administration in healthy volunteers. J Clin Pharmacol 2007;47(1):13-8.
-
Quadir M, Zia H, Needham TE. Development and evaluation of nasal formulations of ketorolac. Drug Deliv 2000;7(4):223-9.
-
Brown C, Moodie J, Bisley E, Bynum L. Intranasal ketorolac for postoperative pain: a phase 3, double-blind, randomized study. Pain Med 2009;10(6):1106-14.
-
Moodie JE, Brown CR, Bisley EJ, Weber HU, Bynum L. The safety and analgesic efficacy of intranasal ketorolac in patients with postoperative pain. Anesth Analg 2008;107(6):2025-31.
-
Singla N, Singla S, Minkowitz HS, Moodie J, Brown C. Intranasal ketorolac for acute postoperative pain. Curr Med Res Opin 2010;26(8):1915-23.
-
Grant GM, Mehlisch DR. Intranasal ketorolac for pain secondary to third molar impaction surgery: a randomized, double-blind, placebo-controlled trial. J Oral Maxillofac Surg 2010;68(5):1025-31.
-
Lundeberg, S. and J.A. Roelofse, Aspects of pharmacokinetics and pharmacodynamics of sufentanil in pediatric practice. Paediatr Anaesth, 2010.
-
Middleton, P.M., et al., Effectiveness of morphine, fentanyl, and methoxyflurane in the prehospital setting. Prehosp Emerg Care, 2010. 14(4): p. 439-47.
-
Bendall, J. C., P. M. Simpson, et al. (2011). "Effectiveness of Prehospital Morphine, Fentanyl, and Methoxyflurane in Pediatric Patients." Prehosp Emerg Care.
-
Rampersad, S., et al., Two-agent analgesia versus acetaminophen in children having bilateral myringotomies and tubes surgery. Paediatr Anaesth, 2010. 20(11): p. 1028-35.
-
Reid, C., R. Hatton, et al. (2011). "Case report: prehospital use of intranasal ketamine for paediatric burn injury." Emerg Med J 28(4): 328-329.
-
Borland, M., S. Milsom, and A. Esson, Equivalency of two concentrations of fentanyl administered by the intranasal route for acute analgesia in children in a paediatric emergency department: A randomized controlled trial. Emerg Med Australas, 2011. 23(2): p. 202-8.
-
Mudd, S., Intranasal Fentanyl for Pain Management in Children: A Systematic Review of the Literature. J Pediatr Health Care, 2011. 25(5): p. 316-22.
-
Pestieau, S.R., et al., The effect of dexmedetomidine during myringotomy and pressure-equalizing tube placement in children. Paediatr Anaesth, 2011. 21(11): p. 1128-35.
-
Steenblik, J., et al., Intranasal sufentanil for the treatment of acute pain in a winter resort clinic. Am J Emerg Med, 2012.
-
Hippard, H. K., K. Govindan, et al. (2012). "Postoperative analgesic and behavioral effects of intranasal fentanyl, intravenous morphine, and intramuscular morphine in pediatric patients undergoing bilateral myringotomy and placement of ventilating tubes." Anesth Analg 115(2): 356-363.
-
Regan, L., A. R. Chapman, et al. (2012). "Nose and vein, speed and pain: comparing the use of intranasal diamorphine and intravenous morphine in a Scottish paediatric emergency department." Emerg Med J.
-
Stephen, R., E. Lingenfelter, et al. (2012). "Intranasal sufentanil provides adequate analgesia for emergency department patients with extremity injuries." J Opioid Manag 8(4): 237-241.
-
Harlos, M. S., S. Stenekes, et al. (2012). "Intranasal Fentanyl in the Palliative Care of Newborns and Infants." J Pain Symptom Manage.
-
Kaube, H., et al., Aura in some patients with familial hemiplegic migraine can be stopped by intranasal ketamine. Neurology, 2000. 55(1): p. 139-41.
-
Christensen, K., et al., Safety and efficacy of intranasal ketamine for acute postoperative pain. Acute pain, 2007. 9: p. 183-192.
-
Reid, C., R. Hatton, and P. Middleton, Case report: prehospital use of intranasal ketamine for paediatric burn injury. Emerg Med J, 2011. 28(4): p. 328-9.
-
Goudas, L.C., et al., Efficacy and safety of intranasal ketamine for the management of breakthrough pain in chronic pain. A randomized, double-blind, placebo-controlled, cross-over trial. American Society of Clinical Oncology Meeting, 2002. Abstract No: 450.
-
Kronenberg, R.H., Ketamine as an analgesic: parenteral, oral, rectal, subcutaneous, transdermal and intranasal administration. J Pain Palliat Care Pharmacother, 2002. 16(3): p. 27-35.
-
Afridi, S. K., N. J. Giffin, et al. (2013). "A randomized controlled trial of intranasal ketamine in migraine with prolonged aura." Neurology 80(7): 642-647.
Abdell-Ghaffar, H. and M. A. M. Salem (2012). "Safety and Analgesic
efficacy of Pre-emptive Intranasal Ketamine versus Intranasal fentanyl
in patients undergoing endoscopic nasal surgery." Journal Am Sci
8(3): 430-436.
Yeaman, F., E. Oakley, et al.
(2013). "Sub-dissociative dose intranasal ketamine for limb injury pain
in children in the emergency department: A pilot study." Emerg Med
Australas 25(2): 161-167.
Gracia, M. R., L. C. Hortelano, et al. (2013). "Intoxicación
accidental por
fentanilo intranasal." Anales de Pediatria
In press.
Johansson J, Sjoberg J, Nordgren M, Sandstrom E, Sjoberg F, Zetterstrom H.
Prehospital analgesia using nasal administration of S-ketamine--a case
series. Scandinavian journal of trauma, resuscitation and emergency
medicine 2013;21:38.
Andolfatto, G., E. Willman, et al. (2013). "Intranasal Ketamine for
Analgesia in the Emergency Department: A Prospective Observational
Series." Acad Emerg Med 20(10):
1050-1054.
Ellerton, J. A., M. Greene, et al. (2013). "The use of analgesia in
mountain rescue casualties with moderate or severe pain." Emerg Med J.
O'Donnell, D. P., L. C. Schafer, et al. (2013). "Effect of Introducing the
Mucosal Atomization Device for Fentanyl Use in Out-of-Hospital Pediatric
Trauma Patients." Prehosp Disaster Med
28(5): 520-522.
Williams, S. (2013). "Nurse initiated intranasal fentanyl to improve the
time to analgesia for children presenting to emergency with suspected
limb fracture." 24th International Nursing research Conference -
Czech Republic July 2013.
Kendall, J., I. Maconochie, et al. (2014). "A novel multipatient
intranasal diamorphine spray for use in acute pain in children:
pharmacovigilance data from an observational study." Emerg Med J.
Karlsen, A.P., et al., Safety of intranasal fentanyl in the out-of-hospital setting: a prospective observational study. Ann Emerg Med, 2014. 63(6): p. 699-703.
Nielsen, B.N., et al., Intranasal sufentanil/ketamine analgesia in children. Paediatr Anaesth, 2014. 24(2): p. 170-80.
Telfer, P., et al., Management of the acute painful crisis in sickle cell disease- a re-evaluation of the use of opioids in adult patients. Br J Haematol, 2014. 166(2): p. 157-64.
Tsze, D.S., et al., Treatment of tetralogy of Fallot hypoxic spell with intranasal fentanyl. Pediatrics, 2014. 134(1): p. e266-9.
Liang, P., et al., Single-dose sufentanil or fentanyl reduces agitation after sevoflurane anesthesia in children undergoing ophthalmology surgery. Pak J Med Sci, 2014. 30(5): p. 1059-63.
Maroli, S., et al., Sniffing out pain: An in vivo intranasal study of analgesic efficacy. J Int Oral Health, 2014. 6(1): p. 66-71.
Sokoloff, C., et al., Is adequate pain relief and time to analgesia associated with emergency department length of stay? A retrospective study. BMJ Open, 2014. 4(3): p. e004288.
Fleet J, Belan I, Jones M, Ullah S, Cyna A. A comparison of fentanyl with pethidine for pain relief during childbirth: a randomised controlled trial. BJOG : an international journal of obstetrics and gynaecology 2015.
Riediger, C., M. Haschke, et al. (2015). "The analgesic effect of combined
treatment with intranasal S-ketamine and intranasal midazolam
compared with morphine patient-controlled analgesia in spinal
surgery patients: a pilot study." J Pain Res
8: 87-94.
Schacherer, N. M., D. E. Ramirez, et al. (2015). "Expedited Delivery of
Pain Medication for Long-Bone Fractures Using an Intranasal Fentanyl
Clinical Pathway." Pediatr Emerg Care.
Dolatabadi, A. A., M. Shojaee, et al. (2015). "Intranasal sufentanil versus intravenous morphine sulfate in pain management of patients with extremity trauma." Iranian Journal of Emergency Medicine 3(2): 116-121.
Graudins, A., R. Meek, et al. (2015). "The PICHFORK (Pain in Children
Fentanyl or Ketamine) trial: a randomized controlled trial comparing
intranasal ketamine and fentanyl for the relief of moderate to
severe pain in children with limb injuries." Ann Emerg Med
65(3): 248-254 e241.
Kerr, D., D. Taylor, et al. (2015). "Patient-controlled intranasal fentanyl
analgesia: a pilot study to assess practicality and tolerability
during childbirth." Int J Obstet Anesth
24(2): 117-123.
Kavanagh, P. L., P. G. Sprinz, et al. (2015). "Improving the
Management of Vaso-Occlusive Episodes in the Pediatric Emergency
Department." Pediatrics
136(4): e1016-1025.
Fein, D. M., J. R. Avner, et al. (2017). "Intranasal fentanyl for initial
treatment of vaso-occlusive crisis in sickle cell disease."
Pediatr Blood Cancer 64(6).
Akinsola B.T., Hagbon R., Zmitrovich A., et al: More rapid delivery of parenteral analgesia by adding intranasal fentnaly8 to the management of sickle cell disease Vaso-occlusive pain.
Barrett, M. J., J. Cronin, et al. (2012). "Intranasal fentanyl
versus intravenous morphine in the emergency department treatment of
severe painful sickle cell crises in children: study protocol for a
randomised controlled trial." Trials
13: 74.
Chew, K. S. and A. H. Shaharudin (2016). "An open-label randomised
controlled trial on the efficacy of adding intranasal fentanyl to
intravenous tramadol in patients with moderate to severe pain
following acute musculoskeletal injuries." Singapore Med J.
Fenster, D. B., P. S. Dayan, et al. (2016). "Randomized Trial of
Intranasal Fentanyl Versus Intravenous Morphine for Abscess Incision
and Drainage." Pediatr Emerg Care.
Kurien, T., K. R. Price, et al. (2016). "Manipulation and reduction of paediatric fractures of the distal radius and forearm using intranasal diamorphine and 50% oxygen and nitrous oxide in the emergency department: a 2.5-year study." Bone Joint J 98-B(1): 131-136.
Murphy, A. P., M. Hughes, et al. (2016). "Intranasal fentanyl for
the prehospital management of acute pain in children." Eur J
Emerg Med.
Phillips, M. L., B. C. Willis, et al. (2016). "Bimodal analgesia vs
fentanyl in pediatric patients undergoing bilateral myringotomy and
tympanostomy tube placement: a propensity matched cohort study."
J Clin Anesth 32:
162-168.
Singh, R., A. Pareek, et al. (2016). "Post-operative analgesic
efficacy of fentanyl via different routes – A comparative study of
nebulisation, intranasal and intravenous routes." IAIM
3(6): 16-22.
Shrestha, R., S. Pant, et al. (2016). "Intranasal ketamine for the
treatment of patients with acute pain in the emergency department."
World J Emerg Med 7(1):
19-24.
Farnia, M. R., A. Jalali, et al. (2017). "Comparison of intranasal ketamine
versus IV morphine in reducing pain in patients with renal colic."
Am J Emerg Med 35(3):
434-437.
Fleet, J. A., M. Jones, et al. (2017). "Taking the alternative route:
Women's experience of intranasal fentanyl, subcutaneous fentanyl or
intramuscular pethidine for labour analgesia." Midwifery
53: 15-19.
Hoeffe, J., E. Doyon Trottier, et al. (2017). "Intranasal fentanyl and
inhaled nitrous oxide for fracture reduction: The FAN observational
study." Am J Emerg Med
35(5): 710-715.
Parvizrad, R., A. Pakniyat, et al. (2017). "Comparing the analgesic effect
of intranasal with intravenous ketamine in isolated orthopedic
trauma: A randomized clinical trial." Turk J Emerg Med
17(3): 99-103.
Reynolds, S. L., K. K. Bryant, et al. (2017). "Randomized Controlled
Feasibility Trial of Intranasal Ketamine Compared to Intranasal
Fentanyl for Analgesia in Children with Suspected Extremity
Fractures." Acad Emerg Med.
Scheier, E., A. Siman, et al. (2017). "Intranasal ketamine proved feasible
for pain control in paediatric care and parental support was high."
Acta Paediatr 106(10):
1702.
Nemeth, M., N. Jacobsen, et al. (2017). "Intranasal Analgesia and
Sedation in Pediatric Emergency Care-A Prospective Observational
Study on the Implementation of an Institutional Protocol in a
Tertiary Children's Hospital." Pediatr Emerg Care.
Akinsola, B., R. Hagbom, et al. (2018). "Impact of Intranasal Fentanyl in Nurse Initiated Protocols for Sickle Cell Vaso-occlusive Pain Episodes in a Pediatric Emergency Department." Am J Hematol.
Kelly, G. S., R. W. Stewart, et al. (2018). "Intranasal fentanyl improves time to analgesic delivery in sickle cell pain crises." Am J Emerg Med 36(7): 1305-1307.
Arnautovic, T., K. Sommese, et al. (2018). "Evaluating the
Implementation Barriers of an Intranasal Fentanyl Pain Pathway for
Pediatric Long-Bone Fractures." Pediatr Emerg Care
34(7): 473-478.
Fenster, D. B., P. S. Dayan, et al. (2018). "Randomized Trial of
Intranasal Fentanyl Versus Intravenous Morphine for Abscess Incision
and Drainage." Pediatr Emerg Care
34(9): 607-612.
Frey, T. M., T. A. Florin, et al. (2018). "Effect of Intranasal
Ketamine vs Fentanyl on Pain Reduction for Extremity Injuries in
Children: The PRIME Randomized Clinical Trial." JAMA Pediatr.
Nejati, A., M. Jalili, et al. (2018). "Intranasal ketamine reduces
pain of digital nerve block; a double blind randomized clinical
trial." Am J Emerg Med.
McHale, B., C. D. Badenhorst, et al. (2018). "Do children undergoing
bilateral myringotomy with placement of ventilating tubes benefit
from pre-operative analgesia? A double-blinded, randomised,
placebo-controlled trial." J Laryngol Otol
132(8): 685-692.
Yenigun, A., S. Yilmaz, et al. (2018). "Demonstration of analgesic
effect of intranasal ketamine and intranasal fentanyl for
postoperative pain after pediatric tonsillectomy." Int J Pediatr
Otorhinolaryngol 104: 182-185.
Kim,
K. S., N. K. Yeo, et al. (2018). "Effect of Fentanyl Nasal Packing
Treatment on Patients With Acute Postoperative Pain After Nasal
Operation: A Randomized Double-Blind Controlled Trial." Ann Otol
Rhinol Laryngol 127(5): 297-305.
Quinn, K., S. Kriss, et al. (2018). "Analgesic Efficacy of
Intranasal Ketamine Versus Intranasal Fentanyl for Moderate to
Severe Pain in Children: A Prospective, Randomized, Double-Blind
Study." Pediatr Emerg Care.
Frey, T. M., T. A. Florin, et al. (2019). "Effect of Intranasal
Ketamine vs Fentanyl on Pain Reduction for Extremity Injuries in
Children: The PRIME Randomized Clinical Trial." JAMA Pediatr
173(2): 140-146.
Guthrie, A. M., R. A. Baum, et al. (2019). "Use of Intranasal
Ketamine in Pediatric Patients in the Emergency Department."
Pediatr Emerg Care.
Lord, B., P. A. Jennings, et al. (2019). "Effects of the
Introduction of Intranasal Fentanyl on Reduction of Pain Severity
Score in Children: An Interrupted Time-Series Analysis." Pediatr
Emerg Care 35(11): 749-754.
Miguez, M. C., C. Ferrero, et al. (2019). "Retrospective Comparison
of Intranasal Fentanyl and Inhaled Nitrous Oxide to Intravenous
Ketamine and Midazolam for Painful Orthopedic Procedures in a
Pediatric Emergency Department." Pediatr Emerg Care.
Williams, J. M., S. Schuman, et al. (2019). "Intranasal Fentanyl and
Midazolam for Procedural Analgesia and Anxiolysis in Pediatric
Urgent Care Centers." Pediatr Emerg Care.
Benish, T., D. Villalobos, et al. (2019). "The THINK (Treatment of
Headache with Intranasal Ketamine) Trial: A Randomized Controlled
Trial Comparing Intranasal Ketamine with Intravenous Metoclopramide."
J Emerg Med 56(3):
248-257 e241.
Turner, A. L., S. Shandley, et al. (2019). "Intranasal Ketamine for
Abortive Migraine Therapy in Pediatric Patients: A Single-Center
Review." Pediatr Neurol.
Blancher, M., M. Maignan, et al. (2019). "Intranasal sufentanil
versus intravenous morphine for acute severe trauma pain: A
double-blind randomized non-inferiority study." PLoS Med
16(7): e1002849.
Lemoel, F., J. Contenti, et al. (2019). "Intranasal sufentanil given
in the emergency department triage zone for severe acute traumatic
pain: a randomized double-blind controlled trial." Intern Emerg
Med 14(4): 571-579.
Mozafari, J., M. Maleki Verki, et al. (2019). "Comparing intranasal
ketamine with intravenous fentanyl in reducing pain in patients with
renal colic: A double-blind randomized clinical trial." Am J
Emerg Med.
Nazemian, N., M. Torabi, et al. (2019). "Atomized intranasal vs
intravenous fentanyl in severe renal colic pain management: A
randomized single-blinded clinical trial." Am J Emerg Med:
158483.
Nejati, A., M. Jalili, et al. (2019). "Intranasal ketamine reduces
pain of digital nerve block; a double blind randomized clinical
trial." Am J Emerg Med
37(9): 1622-1626.
Sin, B., I. Jeffrey, et al. (2019). "Intranasal Sufentanil Versus Intravenous Morphine for Acute Pain in the Emergency Department: A Randomized Pilot Trial." J Emerg Med 56(3): 301-307
Andolfatto, G., K. Innes, et al. (2019). "Prehospital Analgesia With
Intranasal Ketamine (PAIN-K): A Randomized Double-Blind Trial in
Adults." Ann Emerg Med
74(2): 241-250.
Sindhur, M., H. Balasubramanian, et al. (2020). "Intranasal fentanyl
for pain management during screening for retinopathy of prematurity
in preterm infants: a randomized controlled trial." J Perinatol
40(6): 881-887.
Turner, A. L., S. Shandley, et al. (2020). "Intranasal Ketamine for
Abortive Migraine Therapy in Pediatric Patients: A Single-Center
Review." Pediatr Neurol
104: 46-53.
Bouida, W., K. Bel Haj Ali, et al. (2020). "Effect on Opioids
Requirement of Early Administration of Intranasal Ketamine for Acute
Traumatic Pain." Clin J Pain
36(6): 458-462.
Nazemian, N., M. Torabi, et al. (2020). "Atomized intranasal vs
intravenous fentanyl in severe renal colic pain management: A
randomized single-blinded clinical trial." Am J Emerg Med
38(8): 1635-1640.
Pouraghaei, M., P. Moharamzadeh, et al. (2020). "Intranasal ketamine
versus intravenous morphine for pain management in patients with
renal colic: a double-blind, randomized, controlled trial." World
J Urol.
Tanguay, A., J. Lebon, et al. (2020). "Intranasal Fentanyl versus
Subcutaneous Fentanyl for Pain Management in Prehospital Patients
with Acute Pain: A Retrospective Analysis." Prehosp Emerg Care
24(6): 760-768.
Myrick, R., S. Blakemore, et al. (2020). "Outpatient pain clinic and
intranasal fentanyl to improve sickle cell disease outcomes."
Pediatr Blood Cancer 67(10):
e28648.
Paquin, H., E. D. Trottier, et al. (2020). "Evaluation of a clinical
protocol using intranasal fentanyl for treatment of vaso-occlusive
crisis in sickle cell patients in the emergency department."
Paediatr Child Health 25(5):
293-299.