 Therapeutic
Intranasal Drug Delivery
Therapeutic
Intranasal Drug DeliveryFeatured new articles related to intranasal drug delivery:
July - Sept 2011
Klein, E.J., et al., A Randomized Clinical Trial Comparing Oral, Aerosolized Intranasal, and Aerosolized Buccal Midazolam. Ann Emerg Med, 2011.
Abstract: STUDY OBJECTIVE: We determine whether aerosolized intranasal or buccal midazolam reduces the distress of pediatric laceration repair compared with oral midazolam. METHODS: Children aged 0.5 to 7 years and needing nonparenteral sedation for laceration repair were randomized to receive oral, aerosolized intranasal, or aerosolized buccal midazolam. Patient distress was rated by blinded review of videotapes, using the Children's Hospital of Eastern Ontario Pain Score. Secondary outcomes included activity scores, sedation adequacy, sedation onset, satisfaction, and adverse events. RESULTS: For the 169 subjects (median age 3.1 years) evaluated for the primary outcome, we found significantly less distress in the buccal midazolam group compared with the oral route group (P=.04; difference -2; 95% confidence interval -4 to 0) and a corresponding nonsignificant trend for the intranasal route (P=.08; difference -1; 95% confidence interval -3 to 1). Secondary outcomes (177 subjects) favored the intranasal group, including a greater proportion of patients with an optimal activity score (74%), a greater proportion of parents wanting this sedation in the future, and faster sedation onset. Intranasal was the route least tolerated at administration. Adverse events were similar between groups. CONCLUSION: When comparing the administration of midazolam by 3 routes to facilitate pediatric laceration repair, we observed slightly less distress in the aerosolized buccal group. The intranasal route demonstrated a greater proportion of patients with optimal activity scores, greater proportions of parents wanting similar sedation in the future, and faster onset but was also the most poorly tolerated at administration. Aerosolized buccal or intranasal midazolam represents an effective and useful alternative to oral midazolam for sedation for laceration repair.
Web site Editorial comments:
Here is a well designed RCT noting more rapid onset of action and superior sedation when midazolam was given intranasally versus buccally or orally. As noted in almost all studies, the intranasal route burned with administration and caused more discomfort. However, as has been noted by other authors this burning is easily overcome by pretreatment with topical lidocaine (one article by Chiaretti reviewed a few months ago on this web site - click here to that section).
A final comment - having used this therapy now for 20 years and recently having added lidocaine to the regimen I suggest you deliver the lidocaine about 5-10 minutes in advance of the midazolam using 2-4% solution about 0.2 to 0.3 ml per nostril so it has time to take effect. Do not give the midazolam until a few minutes before the laceration repair - you will get mild onset in about 5 minutes, peak in 10-20 and it is going away fast after 25 minutes so time your procedure to fit into that time frame. You will typically only get mild sedation - they still are easily aroused and still will need restraint to suture and will cry some but usually much less than if you do not use the sedative.
Link to a YouTube video review on the doctors network (click here)
Review of this study by English physician (click here)
Lidocaine eliminates the burning and bitter taste associated with intranasal midazolam link.
Pubmed link: http://www.ncbi.nlm.nih.gov/pubmed/21689865
___________________________________
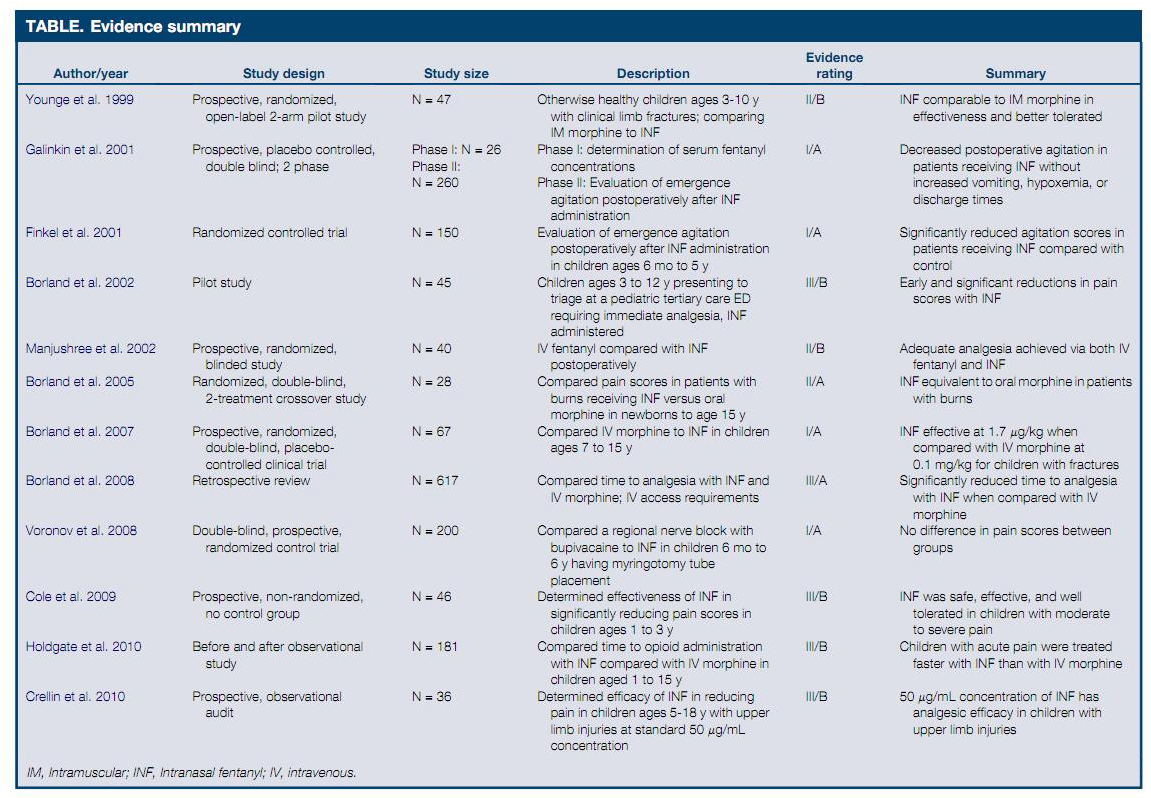
Mudd, S., Intranasal Fentanyl for Pain Management in Children: A Systematic Review of the Literature. J Pediatr Health Care, 2011. 25(5): p. 316-22
Abstract: Intranasally administered fentanyl (INF) has been studied as an alternate route of delivery for pain relief in children. The purpose of this systematic review is to evaluate the available research evidence on the use of INF in the pediatric population. A search was conducted of PubMed, ISI, Scopus, Popline, CINAHL, and Embase for research studies evaluating INF in this population (0-18 years of age). The studies were graded on the strength of the evidence and the results reviewed. All of the reviewed studies showed similar or improved pain scores when compared with other opioids and administration methods. No severe adverse outcomes were reported. Current evidence suggests that INF is a safe and effective method of pain management for children in a variety of clinical settings.
{kind=link}
Web site Editorial comments:
This review provides extensive references (almost all which are also found in the pain section of this web site) to defend its conclusions. The conclusions are that IN fentanyl is equivalent or superior to morphine administered IV, IM or orally and that it is much faster in onset. Furthermore it is safe and does not require compounding (generic 50 ug/ml is fine for children). Given this efficacy, safety and low cost it offers an approach to improve care, improve satisfaction and reduce resource utilization.
Pubmed link: http://www.ncbi.nlm.nih.gov/pubmed/21867860?dopt=Citation
___________________________________
Cheung, C.W., et al., Analgesic and sedative effects of intranasal dexmedetomidine in third molar surgery under local anaesthesia. Br J Anaesth, 2011. 107(3): p. 430-7.
Abstract: BACKGROUND: Dexmedetomidine (DEX) is an alpha 2-adrenoreceptor agonist, which induces sedation and analgesia. This study aimed to determine whether intranasal DEX offered perioperative sedation and better postoperative analgesia. METHODS: Patients having unilateral third molar surgery under local anaesthesia were recruited and allocated to receive either intranasal DEX 1 microg kg(-1) (Group D) or same volume of saline (Group P) 45 min before surgery. Patient-controlled sedation with propofol was offered as a rescue sedative. Perioperative sedation, postoperative pain relief and analgesic consumption, vital signs, adverse events, postoperative recovery, and satisfaction in sedation and analgesia were assessed. RESULTS: Thirty patients from each group were studied. Areas under curve (AUC) of postoperative numerical rating scale (NRS) pain scores 1-12 h at rest and during mouth opening were significantly lower in Group D (P=0.003 and 0.009, respectively). AUC BIS values and OAA/S sedation scores were significantly lower before surgery and at the recovery area (all P<0.01) with significantly less intra-operative propofol used in group D (P<0.01). In group D, heart rate was significantly lower at recovery period (P=0.005) while systolic blood pressure in different periods of the study (all P<0.01), but the decreases did not require treatment. More patients from placebo group experienced dizziness (P=0.026) but no serious adverse event was found. No difference was found in postoperative psychomotor recovery and satisfaction in pain relief and sedation. CONCLUSIONS: Patients receiving intranasal DEX for unilateral third molar surgery with local anaesthesia were more sedated perioperatively with better postoperative pain relief. No delay in psychomotor recovery was seen.
Web site Editorial comments:
This is the first clinical trial using IN dexmedetomidine in adults. The results demonstrate better sedation at the time of surgery, less use of propofol during surgery and better post-operative pain relief. The authors make specific comments regarding the long length of action making it fairly ideal for pre-operative sedation since there is considerable variation between time of delivery and final arrival in the operating suite. Despite this length of action there was no delay in recovery for this type of dental surgical extraction (perhaps this would not be the case for something fast like a myringotomy).
Pubmed link: http://www.ncbi.nlm.nih.gov/pubmed/21685111?dopt=Citation
___________________________________