 Therapeutic
Intranasal Drug Delivery
Therapeutic
Intranasal Drug DeliveryIntranasal medication delivery - brief overview of the concept
Table of Contents
Intranasal drug delivery - General Principles (click here)
Indications for intranasal medication delivery (click here)
Definition of terms
Therapeutic threshold, Side effect threshold (click here)
First Pass metabolism (click here)
Nose Brain pathway (click here)
Why not Buccal or oral rather than intranasal? (click here)
Intranasal drug delivery - General principles
The nasal cavity's easily accessible, rich vascular plexus permits topically administered drugs to rapidly achieve effective blood levels while avoiding intravenous catheters. This is most effectively accomplished by distributing drug solutions as a mist rather than as larger droplets which may aggregate and run off instead of being absorbed.
Because of this easily accessed vascular bed, nasal administration of medications is emerging as a promising method of delivering medications directly to the blood stream. This method of delivery can eliminate the need for intravenous catheters while still achieving rapid, effective blood levels of the medication administered.
Administering medications via the nasal mucosal offers several advantages:
-
The rich vascular plexus of the nasal cavity provides a direct route into the blood stream for medications that easily cross mucous membranes.
-
This direct absorption into the blood stream avoids gastrointestinal destruction and hepatic first pass metabolism (destruction of drugs by liver enzymes) allowing more drug to be cost-effectively, rapidly, and predictably bioavailable than if it were administered orally.
For many IN medications the rates of absorption and plasma concentrations are comparable to intravenous administration, and are typically better than subcutaneous or intramuscular routes.
Ease, convenience and safety: IN drug administration is essentially painless, and does not require sterile technique, intravenous catheters or other invasive devices, and it is immediately and readily available for all patients.
Because the nasal mucosa is nearby the brain, cerebrospinal fluid (CSF) drug concentrations can exceed plasma concentrations. IN administration may rapidly achieve therapeutic brain and spinal cord (CNS) drug concentrations.
Indications for intranasal medication delivery
Intranasal (IN) medication delivery is simply another option or method to deliver therapeutic medications to the patient’s blood stream to achieve a desired clinical effect. It is a tool in the therapeutic armamentarium just as oral, rectal, sublingual, intramuscular and intravenous delivery methods are also tools to deliver medications.
| Delivery Method | Advantages | Disadvantages |
|---|---|---|
| Oral | ●
Painless ● Ease of use ● No shot needed ● Many medications available for this delivery method ● Extended release options allow long time of efficacy |
● Slow onset of action ● Low Bioavailability |
| Rectal | ● Minimal
pain ● No shot needed |
● Variable first pass metabolism
/ bioavailability ● Somewhat slow onset of action ● Socially unacceptable for many patients ● Limited medications that can be delivered in this fashion |
| Buccal/sublingual | ●
Painless ● Ease of use ● No shot needed ● Avoids first pass metabolism - improving bioavailability over oral and rectal doses |
● Relatively small absorptive
mucosal surface area ● Easy to swallow and convert to oral medication ● Compliance in accepting dose difficult in children and some developmentally delayed adults ● Limited medications that can be delivered in this fashion |
| Intranasal | ●
Painless ● Ease of use ● No shot needed ● Avoids first pass metabolism - improving bioavailability over oral and rectal doses ● Nose-brain pathway allows direct delivery to the cerebral spinal fluid ● Compliance not an issue - easy and fast to deliver to any patient |
● Limited medications that can be delivered in this fashion ● Many medications are not adequately concentrated to achieve ideal dosing volumes ● Mucosal health impacts absorption |
| Intramuscular | ●
Traditional and well understood method ● Many medications developed for this delivery method |
● Painful every time ● Requires proper training and technique to use safely - not readily available to the public ● Variable onset of action and bioavailability ● Infection risk ● Needle stick risk |
| Intravenous | ●
Traditional and well understood method ● Many medications developed for this delivery method ● High bioavailability ● The true gold standard to compare all other methods against ● Very rapid and predictable onset of action |
● Painful to
establish ● Requires proper training and technique to use safely - not readily available to the public and sometimes very difficult even for medical providers ● Infection risk ● Needle stick risk |
Point: There are multiple options to deliver medications to patients. The patients individual needs and issues, as well as the medication that one wishes to administer will determine the most appropriate option(s) for providing that medication. In selected cases, IN delivery has many advantages over other options.
Definition of terms
Bioavailability
How much medication that is administered actually ends up in the blood stream at the source tissue to exert a clinical effect. For example, almost all of a medication given intravenously is “bioavailable” since it goes straight into the blood stream. On the other hand, if the medication is given by mouth, most will not be bioavailable in the blood due to destruction by the acid in the stomach, failure to absorb through the gut and finally through destruction by the liver in a process called hepatic “first pass metabolism.” This is why the dose of a medication given intravenously is almost always far less than that given by mouth.
Factors that affect bioavailability
Characteristics of the drug
-
Molecular size, complexity and lipophilicity
-
pH of solution and pKa of the drug
-
Drug concentration/volume of solutions*
-
Properties of the formulation vehicle (absorption enhancers)
In general, medications that consist of small, simple, lipophilic molecules will cross membranes most easily. Having a pH near physiologic helps as well. Finally, if the drug concentration is such that it can be delivered in a reasonable volume to the nose so no runoff into the throat or out the nostril occurs, then more absorption and higher bioavailability is possible.
In general the ideal volume for one nostril is about 0.25 to 0.3 ml, though some clinicians use as much as 1 ml per nostril and accept runoff and drug loss at this higher volume. (See section below for more discussion about drug volume).Mechanical Factors
-
Site and surface area of drug deposition*
-
Method of administration and subsequent particle size and distribution
-
Mechanical drug loss anteriorly and posteriorly
The larger the nasal mucosal surface area that is covered, the more medication that can be absorbed. Ideally, drug doses will be divided in half, and each nostril received half the dose, which doubles the absorptive surface area.[1] In addition, a significant difference in drug distribution is observed when various modes of medication administration are used: nose drops, plastic bottle nebulizer, atomization pump, pressurized aerosol. Multiple studies show that the atomized pump is the best nasal delivery system because it gives a constant dose and a very good mucosal distribution.[2, 3] In addition, research has demonstrated that clearance of spray is much slower than clearance of drops[4] since much of the spray deposits on nonciliated areas, whereas nose drop solutions are primarily distributed on ciliated surfaces. Particle size also affects distribution. With nasal breathing, nearly all particles with a size of 10-20 µm are deposited on the nasal mucosa, those less than 2 µm pass through the nasal cavity and deposit in the lungs.[5, 6] If drugs are introduced as soluble particles they may readily pass into the nasal lining secretions and then be absorbed into the blood.
Anatomic features of the patient
- Blood flow to the nasal mucosa
- Rate of clearance (ciliary activity)
- Pathologic conditions affecting nasal function
If blood flow to the nasal mucosa is poor, absorption of drug will be poor. This can occur in situations where previous events have destroyed the nasal mucosa (trauma, surgery, cocaine induced destruction of the mucosa). Topical vasoconstrictors such as recent "snorting" of cocaine will also dramatically reduce absorption. Finally, if the patient has a bloody nose or large volumes of mucous production, the applied medication is either washed off, or has trouble gaining contact with the nasal mucosa and cannot be absorbed.
Key points concerning bioavailability:
Use the most concentrated form/lowest volume of the medication available – ideal volumes are about 0.25 to 0.3 ml per nostril to reduce runoff but allow maximal mucosal coverage.[1] Use both nostrils to double the absorptive surface area. Deliver the drug as an atomized spray to maximize surface area coverage. Beware of reduced effect in patients with bloody noses or high mucous production in nasal cavity
.Drug volume discussion
The volume of drug administered is a poorly studied but important
clinical concept for those who are interested in a deeper understanding
of intranasal medication delivery and the pharmaceutical/FDA approach to
dosing and concentration versus the approach of clinicians who just want
to help their patients. In order for a pharmaceutical company to get a
nasal medication approved they need to achieve certain parameters set
down by the FDA or other regulatory body. One of those parameters is
often a bioavailability test of the nasal drug when compared to an
already approved method of delivering the same medication such as via
the intramuscular route. For example, the FDA required that
IN naloxone bioavailability
needed to be the same as IM naloxone before they would approve the
commercially available kit released in 2015. This bioavailability was
determined to be 40% compared to the same dose give IV (which for all
intents and purposes is 100% bioavailable). To achieve this
bioavailability there can be NO waste of drug due to run-off (regardless
of whether that waste allows more total drug to be absorbed by giving a
higher mg dose). For this reason nasal drugs are highly concentrated and
packaged into volumes of around 0.1 ml for delivery. You will see
references stating this is the optimal volume clinically but none of the
references I have ever seen actually have compared 0.1 ml to any other
volumes so this statement should not be accepted at face value. In fact
the only study I have ever seen directly comparing volumes was by Aoki
in 1976 and they found no difference between 0.1 and 0.75 ml but the
study was using vaccines particles and is not really applicable to our
question regarding clinical efficacy of various volumes of CNS active
drugs.[15] While this small volume (0.1 ml)when delivered in a volunteer
setting ensures no run-off and high bioavailability, it is not
necessarily optimal for clinical use. Clinicians in the real world want
the best clinical effect which is not the same as the best
bioavailability. Tiny doses (0.1 ml) are hard to deliver and might
accidentally be sprayed onto the nasal ala or septum with little
resulting clinical efficacy. Volumes in the 0.3 to 0.5 range are
clinically easier to deliver, cover a larger surface area and a little
waste is fine as long as the clinical effect is adequate and no
additional side effects occur. Furthermore these larger volumes can be
administered to both nostrils to allow exposure to a larger absorptive
surface. A study by Tsze et al study confirms this concept in the real
world and found that the volumes of 0.5 ml
or 1 ml volume are easier to use
and preferred by clinicians to a 0.2ml volume.[16] However, its findings
are also debatable because they did not give a single dose of 0.2, 0.5
or 1 ml with variable concentrations. Instead they
gave the same weight based volume
of the drug to each child but varied the number of administrations using
0.2, 0.5 or 1.0 ml aliquots. Perhaps
a future study will be able to concentrate the IN medication into
multiple concentrations (similar to how diamorphine is administered –
starting with lyophylized powder and solubilizing it with three
different volumes having identical drug doses, then testing that
method.)
Therapeutic threshold, Side effect threshold
A common problem with IN medication delivery is that the clinician fails to give an adequate dose of the drug because they are used to using IV medications and are afraid to give a seemingly very high dose of "IV" medication via the nose. For example, to sedate a child for a procedure one needs 0.4 to 0.5 mg/kg of midazolam intranasally. In a 20 kg child that comes out to 10 mg of medication – a seemingly huge dose. Failure to use adequate dosing will lead to inability to achieve a therapeutic threshold and the patient will not have adequate effect from the medication. To understand the reasoning behind administering such "high" doses one must consider several factors. The first is bioavailability. For oral medications we often give 10 to 100 times higher doses of a medication – because it takes that much to achieve adequate blood levels. For IN medications the doses are not that high, but they do need to be more than IV doses to achieve adequate serum levels of medication. How much more will depend on the medication bioavailability.
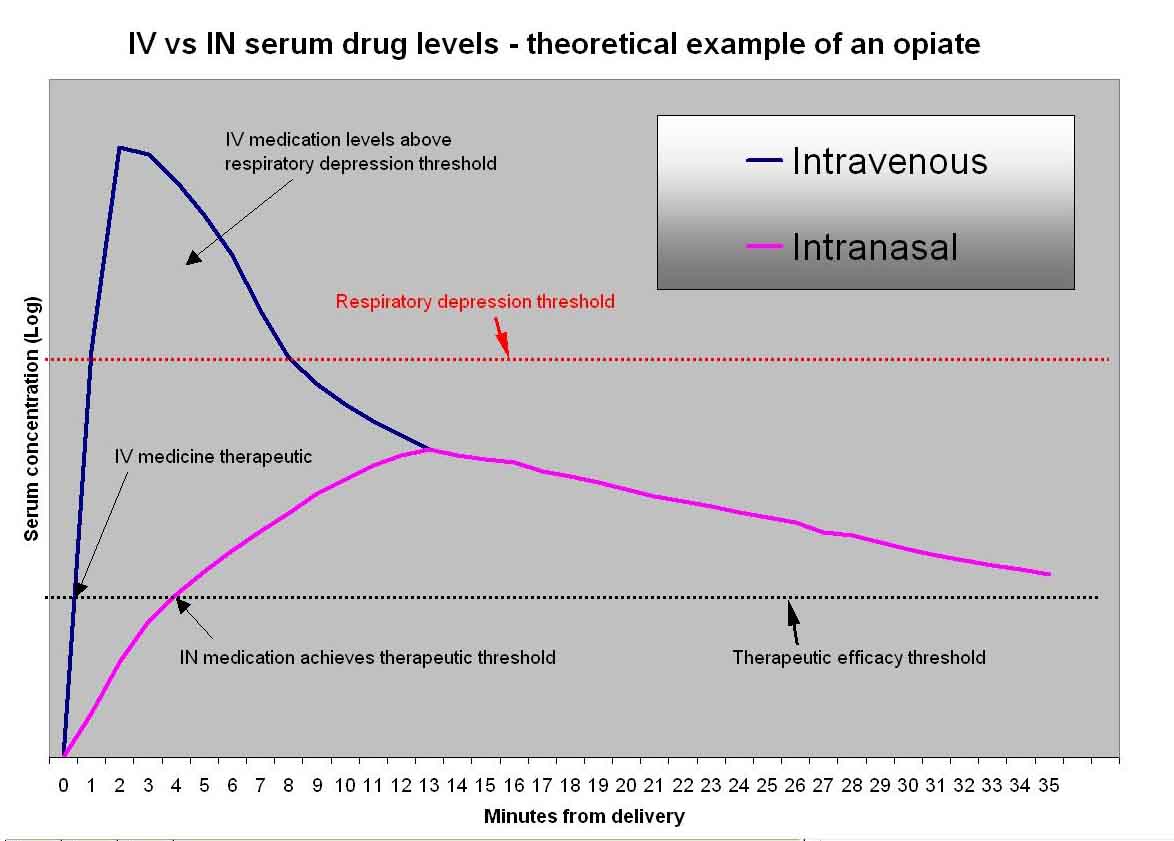
Secondly, the medication is not instantly in the serum when given via the IN route (as is the case with IV medication). It takes several minutes to absorb, often achieving therapeutic effect in 3-5 minutes and peaking at 10-15 minutes. Due to this delayed rise, IN medications given in proper doses will rarely achieve levels high enough to cause clinically important respiratory depression. The exception to this rule is when using sufentanil - it is so potent that inadvertent overdosing or administration to a patient who is already altered can result in respiratory depression and even apnea. For this reason be sure to give properly measured doses and to always monitor these patients
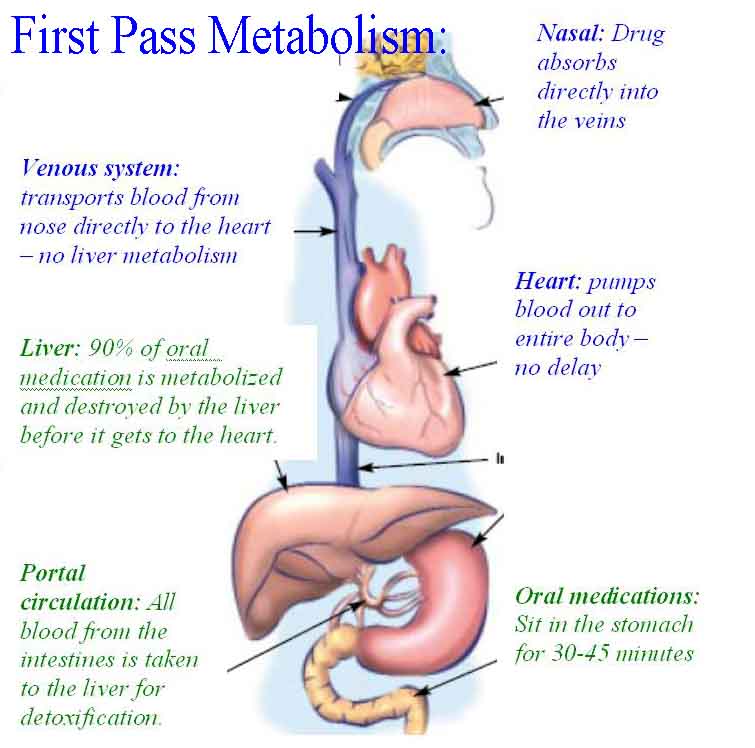
.First Pass metabolism
Almost all molecules absorbed through the gut enter the blood through the "portal" circulation and are transported to the liver on their way into the main blood pool of the body. The liver is full of enzymes that breakdown these molecules (metabolize) and plays an important role in removing toxins from the body. In the case of medications that are taken by mouth, it is common for most of the medication to be destroyed by the liver and never make it into the main blood pool of the body. This destruction by the liver is called "hepatic first pass metabolism". Drugs that are delivered by other routes (IV, IM, SQ, nasal) do not enter the portal circulation and are not subjected to first pass metabolism.
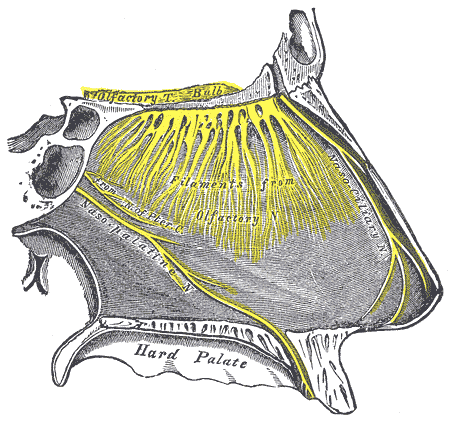
Nose Brain pathway
If the nasally administered medication contacts the olfactory mucosa, there is good evidence that suggests molecule transport can occur directly across this tissue and into the cerebral spinal fluid.[7-10] The olfactory mucosa is located in the upper nasal cavity, just below the cribriform plate of the skull. It contains olfactory cells which traverse the cribriform plate and extend up into the cranial cavity. When medication molecules come in contact with this specialized mucosa they are rapidly transported directly into the brain, skipping the blood-brain barrier, and achieving very rapid cerebrospinal fluid levels (often faster than if the drug is given intravenously). This concept of transfer of molecules from the nose to the brain is referred to as the nose-brain pathway and has implications when centrally acting medications such as sedatives, anti-seizure drugs and opiates are delivered nasally. Multiple authors demonstrate that the nose-brain pathway leads to nearly immediate delivery of some nasal medications to the cerebral spinal fluid, by-passing the blood brain barrier.[7-10]
Lipophilicity
"Lipid loving" - implies that the molecule will easily absorb and cross a lipid membrane. Cell membranes are made of lipids. A molecule with high lipophilicity will easily cross cell membranes (mucous membranes, vascular membranes, blood brain barrier) and enter the blood stream and cerebral spinal fluid.
Why not Buccal or oral rather than intranasal?
The most common reason one would not choose an oral route and would instead elect to use nasal or buccal routes is due to delays in onset of oral medications and due to gastric acid destruction and first pass metabolism of drug resulting in very low levels available to the blood stream. Failure to utilize the nose brain path also occurs with oral (and buccal) medications - resulting in much slower drug delivery to the brain. Interestingly, oral medications are also commonly refused by 30% of pediatric patients making them completely ineffective in this situation.[11] Buccal medications also require a cooperative patient who will retain the medication within their buccal and sublingual mucosal areas and not swallow or spit it out. In fact, even when buccal medications are administered to volunteers in research settings, only about 56% remains in the oral cavity for absorption.[12] Even nasal drug delivery can have problems depending on the delivery method. Yuen et al report that in 5.3% of pediatric patients they were unable to dispense drops into the nose due to resistance to this delivery technique.[13] While nasal delivery is possible the majority of the time, to overcome these delivery issues a number of device have been developed that enhance delivery - these are discussed in the delivery techniques section of this web site.
Bibliography (click here for full abstracts)
-
Dale, O., R. Hjortkjaer, and E.D. Kharasch, Nasal administration of opioids for pain management in adults. Acta Anaesthesiol Scand, 2002. 46(7): p. 759-70.
-
Mygind, N. and S. Vesterhauge, Aerosol distribution in the nose. Rhinology, 1978. 16(2): p. 79-88.
-
Mygind, N., Nasal Allergy, 2nd edition. Blackwell, Oxford, England, 1979: p. 257-270.
-
Hardy, J.G., S.W. Lee, and C.G. Wilson, Intranasal drug delivery by spray and drops. J Pharm Pharmacol, 1985. 37(5): p. 294-7.
-
Hatch, T.F., Distribution and deposition of the inhaled particles in respiratory tract. Bact Rev, 1961. 25: p. 237.
-
Stuart, B.O., Deposition of inhaled aerosols. Arch Intern Med, 1973. 131(1): p. 60-73.
-
Henry, R.J., et al., A pharmacokinetic study of midazolam in dogs: nasal drop vs. atomizer administration. Pediatr Dent, 1998. 20(5): p. 321-6.
-
Sakane, T., et al., Transport of cephalexin to the cerebrospinal fluid directly from the nasal cavity. J Pharm Pharmacol, 1991. 43(6): p. 449-51.
-
Banks, W.A., M.J. During, and M.L. Niehoff, Brain uptake of the glucagon-like peptide-1 antagonist exendin(9-39) after intranasal administration. J Pharmacol Exp Ther, 2004. 309(2): p. 469-75.
-
Westin, et al., Direct nose-to-brain transfer of morphine after nasal administration to rats. Pharm Res, 2006. 23(3): p. 565-72.
-
Khalil, S., H. Vije, and S. Kee, A paediatric trial comparing midazolam/syrpalta mixture with premixed midazolam syrup (Roche). Paediatr Anaesth, 2003. 13: p. 205-209.
-
Anttila, M., et al., Bioavailability of dexmedetomidine after extravascular doses in healthy subjects. Br. J Clin Pharmacol, 2003. 56: p. 691-693.
-
Yuen, V.M., et al., A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial. Anesth Analg, 2008. 106(6): p. 1715-21.
-
-
Aoki, F. Y. and J. C. Crowley (1976). "Distribution and removal of human serum albumin-technetium 99m instilled intranasally." Br J Clin Pharmacol 3(5): 869-878.
-
Tsze, D. S., M. Ieni, et al. (2017). "Optimal Volume of Administration of Intranasal Midazolam in Children: A Randomized Clinical Trial." Ann Emerg Med 69(5): 600-609.